
Chapter 3: Biopsychology
Introduction
Have you ever taken a device apart to find out how it works? Many of us have done so, whether to attempt a repair or simply to satisfy our curiosity. A device’s internal workings are often distinct from its user interface on the outside. For example, we don’t think about microchips and circuits when we turn up the volume on a mobile phone; instead, we think about getting the volume just right. Similarly, the inner workings of the human body are often distinct from the external expression of those workings. It is the job of psychologists to find the connection between these—for example, to figure out how the firings of millions of neurons become a thought.
This chapter strives to explain the biological mechanisms that underlie behavior. These physiological and anatomical foundations are the basis for many areas of psychology. In this chapter, you will learn how genetics influence both physiological and psychological traits. You will become familiar with the structure and function of the nervous system. And, finally, you will learn how the nervous system interacts with the endocrine system.
Cells of the Nervous System
Learning Objectives
- Identify the basic parts of a neuron
- Describe how neurons communicate with each other
- Explain how drugs act as agonists or antagonists for a given neurotransmitter system
Psychologists striving to understand the human mind may study the nervous system. Learning how the cells and organs (like the brain) function, help us understand the biological basis behind human psychology. The nervous system is composed of two basic cell types: glial cells (also known as glia) and neurons. Glial cells, which outnumber neurons ten to one, are traditionally thought to play a supportive role to neurons, both physically and metabolically. Glial cells provide scaffolding on which the nervous system is built, help neurons line up closely with each other to allow neuronal communication, provide insulation to neurons, transport nutrients and waste products, and mediate immune responses. Neurons, on the other hand, serve as interconnected information processors that are essential for all of the tasks of the nervous system. This section briefly describes the structure and function of neurons.
NEURON STRUCTURE
Neurons are the central building blocks of the nervous system, 100 billion strong at birth. Like all cells, neurons consist of several different parts, each serving a specialized function (Figure 3.8). A neuron’s outer surface is made up of a semipermeable membrane. This membrane allows smaller molecules and molecules without an electrical charge to pass through it, while stopping larger or highly charged molecules.
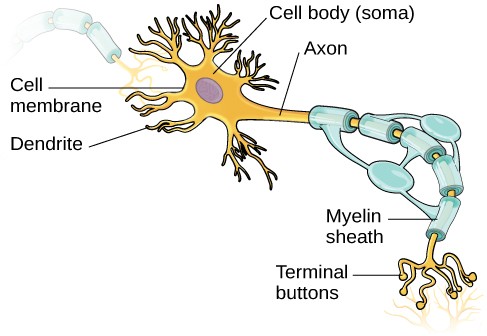
Figure 3.8 This illustration shows a prototypical neuron, which is being myelinated.
The nucleus of the neuron is located in the soma, or cell body. The soma has branching extensions known as dendrites. The neuron is a small information processor, and dendrites serve as input sites where signals are received from other neurons. These signals are transmitted electrically across the soma and down a major extension from the soma known as the axon, which ends at multiple terminal buttons. The terminal buttons contain synaptic vesicles that house neurotransmitters, the chemical messengers of the nervous system.
Axons range in length from a fraction of an inch to several feet. In some axons, glial cells form a fatty substance known as the myelin sheath, which coats the axon and acts as an insulator, increasing the speed at which the signal travels. The myelin sheath is crucial for the normal operation of the neurons within the nervous system: the loss of the insulation it provides can be detrimental to normal function.
In healthy individuals, the neuronal signal moves rapidly down the axon to the terminal buttons, where synaptic vesicles release neurotransmitters into the synapse (Figure3.9). The synapse is a very small space between two neurons and is an important site where communication between neurons occurs. Once neurotransmitters are released into the synapse, they travel across the small space and bind with corresponding receptors on the dendrite of an adjacent neuron. Receptors, proteins on the cell surface where neurotransmitters attach, vary in shape, with different shapes “matching” different neurotransmitters.
How does a neurotransmitter “know” which receptor to bind to? The neurotransmitter and the receptor have what is referred to as a lock-and-key relationship—specific neurotransmitters fit specific receptors similar to how a key fits a lock. The neurotransmitter binds to any receptor that it fits.

Figure 3.9 (a) The synapse is the space between the terminal button of one neuron and the dendrite of another neuron. (b) In this pseudo-colored image from a scanning electron microscope, a terminal button (green) has been opened to reveal the synaptic vesicles (orange and blue) inside. Each vesicle contains about 10,000 neurotransmitter molecules.
NEURONAL COMMUNICATION
Now that we have learned about the basic structures of the neuron and the role that these structures play in neuronal communication, let’s take a closer look at the signal itself—how it moves through the neuron and then jumps to the next neuron, where the process is repeated.
We begin at the neuronal membrane. The neuron exists in a fluid environment—it is surrounded by extracellular fluid and contains intracellular fluid (i.e., cytoplasm). The neuronal membrane keeps these two fluids separate—a critical role because the electrical signal that passes through the neuron depends on the intra- and extracellular fluids being electrically different. This difference in charge across the membrane, called the membrane potential, provides energy for the signal.
The electrical charge of the fluids is caused by charged molecules (ions) dissolved in the fluid. The semipermeable nature of the neuronal membrane somewhat restricts the movement of these charged molecules, and, as a result, some of the charged particles tend to become more concentrated either inside or outside the cell.
Between signals, the neuron membrane’s potential is held in a state of readiness, called the resting potential. Like a rubber band stretched out and waiting to spring into action, ions line up on either side of the cell membrane, ready to rush across the membrane when the neuron goes active and the membrane opens its gates (i.e., a sodium-potassium pump that allows movement of ions across the membrane). Ions in high-concentration areas are ready to move to low-concentration areas, and positive ions are ready to move to areas with a negative charge.
In the resting state, sodium (Na+) is at higher concentrations outside the cell, so it will tend to move into the cell. Potassium (K+), on the other hand, is more concentrated inside the cell, and will tend to move out of the cell (Figure 3.10). In addition, the inside of the cell is slightly negatively charged compared to the outside. This provides an additional force on sodium, causing it to move into the cell.

Figure 3.10 At resting potential, Na+ (blue pentagons) is more highly concentrated outside the cell in the extracellular fluid (shown in blue), whereas K+ (purple squares) is more highly concentrated near the membrane in the cytoplasm or intracellular fluid. Other molecules, such as chloride ions (yellow circles) and negatively charged proteins (brown squares), help contribute to a positive net charge in the extracellular fluid and a negative net charge in the intracellular fluid.
From this resting potential state, the neuron receives a signal and its state changes abruptly (Figure 3.11). When a neuron receives signals at the dendrites—due to neurotransmitters from an adjacent neuron binding to its receptors—small pores, or gates, open on the neuronal membrane, allowing Na+ ions, propelled by both charge and concentration differences, to move into the cell. With this influx of positive ions, the internal charge of the cell becomes more positive. If that charge reaches a certain level, called the threshold of excitation, the neuron becomes active and the action potential begins.
Many additional pores open, causing a massive influx of Na+ ions and a huge positive spike in the membrane potential, the peak action potential. At the peak of the spike, the sodium gates close and the potassium gates open. As positively charged potassium ions leave, the cell quickly begins repolarization. At first, it hyperpolarizes, becoming slightly more negative than the resting potential, and then it levels off, returning to the resting potential.
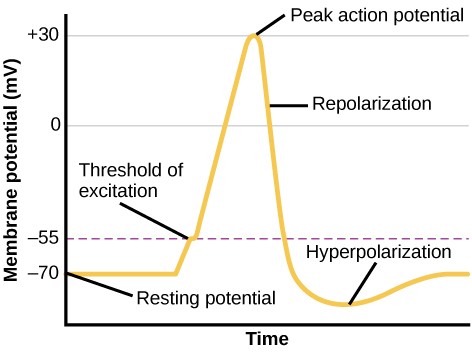
Figure 3.11 During the action potential, the electrical charge across the membrane changes dramatically.
This positive spike constitutes the action potential: the electrical signal that typically moves from the cell body down the axon to the axon terminals. The electrical signal moves down the axon like a wave; at each point, some of the sodium ions that enter the cell diffuse to the next section of the axon, raising the charge past the threshold of excitation and triggering a new influx of sodium ions. The action potential moves all the way down the axon to the terminal buttons.
The action potential is an all-or-none phenomenon. In simple terms, this means that an incoming signal from another neuron is either sufficient or insufficient to reach the threshold of excitation. There is no in- between, and there is no turning off an action potential once it starts. Think of it like sending an email or a text message. You can think about sending it all you want, but the message is not sent until you hit the send button. Furthermore, once you send the message, there is no stopping it.
Because it is all or none, the action potential is recreated, or propagated, at its full strength at every point along the axon. Much like the lit fuse of a firecracker, it does not fade away as it travels down the axon. It is this all-or-none property that explains the fact that your brain perceives an injury to a distant body part like your toe as equally painful as one to your nose.
As noted earlier, when the action potential arrives at the terminal button, the synaptic vesicles release their neurotransmitters into the synapse. The neurotransmitters travel across the synapse and bind to receptors on the dendrites of the adjacent neuron, and the process repeats itself in the new neuron (assuming the signal is sufficiently strong to trigger an action potential). Once the signal is delivered, excess neurotransmitters in the synapse drift away, are broken down into inactive fragments, or are reabsorbed in a process known as reuptake. Reuptake involves the neurotransmitter being pumped back into the neuron that released it, in order to clear the synapse (Figure3.12). Clearing the synapse serves both to provide a clear “on” and “off” state between signals and to regulate the production of neurotransmitter (full synaptic vesicles provide signals that no additional neurotransmitters need to be produced).
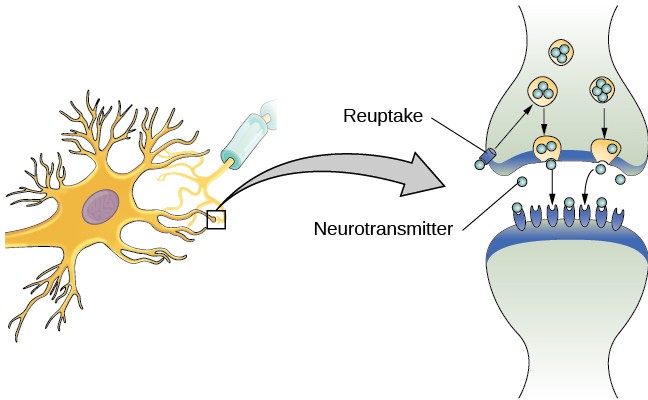
Figure 3.12 Reuptake involves moving a neurotransmitter from the synapse back into the axon terminal from which it was released.
Neuronal communication is often referred to as an electrochemical event. The movement of the action potential down the length of the axon is an electrical event, and movement of the neurotransmitter across the synaptic space represents the chemical portion of the process.
NEUROTRANSMITTERS AND DRUGS
There are several different types of neurotransmitters released by different neurons, and we can speak in broad terms about the kinds of functions associated with different neurotransmitters (Table3.1). Much of what psychologists know about the functions of neurotransmitters comes from research on the effects of drugs in psychological disorders. Psychotropic medications are drugs that treat psychiatric symptoms by restoring neurotransmitter balance.
|
Table 3.1 Major Neurotransmitters and How They Affect Behavior |
||
|
Neurotransmitter |
Involved in |
Potential Effect on Behavior |
|
Acetylcholine |
Muscle action, memory |
Increased arousal, enhanced cognition |
|
Beta-endorphin |
Pain, pleasure |
Decreased anxiety, decreased tension |
|
Dopamine |
Mood, sleep, learning |
Increased pleasure, suppressed appetite |
|
Gamma-aminobutyric acid (GABA) |
Brain function, sleep |
Decreased anxiety, decreased tension |
|
Glutamate |
Memory, learning |
Increased learning, enhanced memory |
|
Norepinephrine |
Heart, intestines, alertness |
Increased arousal, suppressed appetite |
|
Serotonin |
Mood, sleep |
Modulated mood, suppressed appetite |
Psychoactive drugs can act as agonists or antagonists for a given neurotransmitter system. Agonists are chemicals that mimic a neurotransmitter at the receptor site and, thus, strengthen its effects. An antagonist, on the other hand, blocks or impedes the normal activity of a neurotransmitter at the receptor. Agonist and antagonist drugs are prescribed to correct the specific neurotransmitter imbalances underlying a person’s condition. For example, Parkinson’s disease, a progressive nervous system disorder, is associated with low levels of dopamine. Therefore dopamine agonists, which mimic the effects of dopamine by binding to dopamine receptors, are one treatment strategy.
In contrast to agonists and antagonists, which both operate by binding to receptor sites, reuptake inhibitors prevent unused neurotransmitters from being transported back to the neuron. This leaves more neurotransmitters in the synapse for a longer time, increasing its effects. Depression, which has been consistently linked with reduced serotonin levels, is commonly treated with selective serotonin reuptake inhibitors (SSRIs). By preventing reuptake, SSRIs strengthen the effect of serotonin, giving it more time to interact with serotonin receptors on dendrites. Common SSRIs on the market today include Prozac, Paxil, and Zoloft. Individuals vary dramatically in how they respond to the drugs. To improve chances for success, it is not uncommon for people receiving pharmacotherapy to undergo psychological and/or behavioral therapies as well. Some research suggests that combining drug therapy with other forms of therapy tends to be more effective than any one treatment alone.
Parts of the Nervous System
Learning Objectives
- Describe the difference between the central and peripheral nervous systems
- Explain the difference between the somatic and autonomic nervous systems
- Differentiate between the sympathetic and parasympathetic divisions of the autonomic nervous system
The nervous system can be divided into two major subdivisions: the central nervous system (CNS) and the peripheral nervous system (PNS), shown in Figure3.13. The CNS is comprised of the brain and spinal cord; the PNS connects the CNS to the rest of the body. In this section, we focus on the peripheral nervous system; later, we look at the brain and spinal cord.
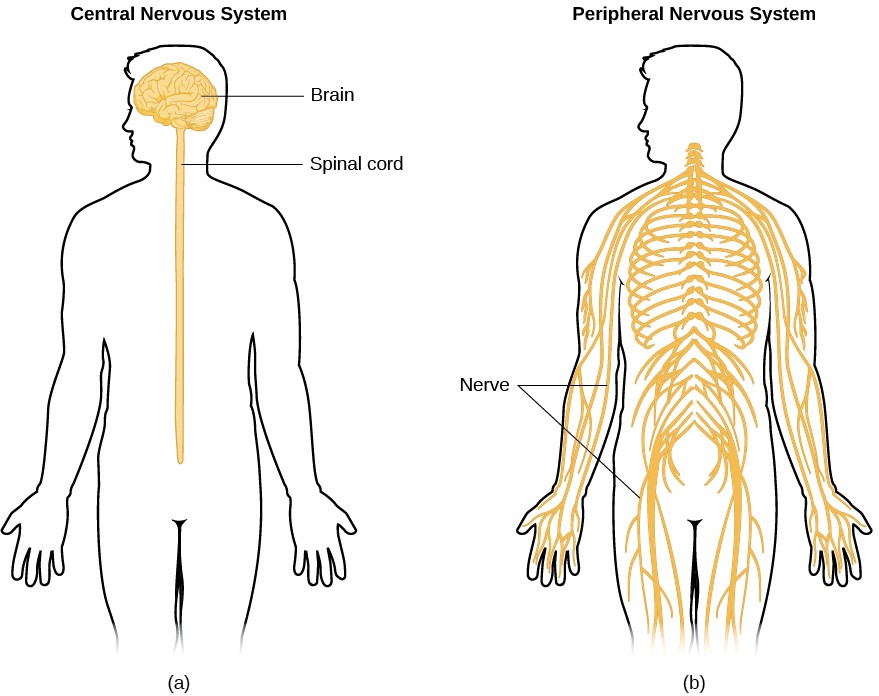
Figure 3.13 The nervous system is divided into two major parts: (a) the Central Nervous System and (b) the Peripheral Nervous System.
PERIPHERAL NERVOUS SYSTEM
The peripheral nervous system is made up of thick bundles of axons, called nerves, carrying messages back and forth between the CNS and the muscles, organs, and senses in the periphery of the body (i.e., everything outside the CNS). The PNS has two major subdivisions: the somatic nervous system and the autonomic nervous system.
The somatic nervous system is associated with activities traditionally thought of as conscious or voluntary. It is involved in the relay of sensory and motor information to and from the CNS; therefore, it consists of motor neurons and sensory neurons. Motor neurons, carrying instructions from the CNS to the muscles, are efferent fibers (efferent means “moving away from”). Sensory neurons, carrying sensory information to the CNS, are afferent fibers (afferent means “moving toward”). Each nerve is basically a two-way superhighway, containing thousands of axons, both efferent and afferent.
The autonomic nervous system controls our internal organs and glands and is generally considered to be outside the realm of voluntary control. It can be further subdivided into the sympathetic and parasympathetic divisions (Figure 3.14). The sympathetic nervous system is involved in preparing the body for stress-related activities; the parasympathetic nervous system is associated with returning the body to routine, day-to-day operations. The two systems have complementary functions, operating in tandem to maintain the body’s homeostasis. Homeostasis is a state of equilibrium, in which biological conditions (such as body temperature) are maintained at optimal levels.
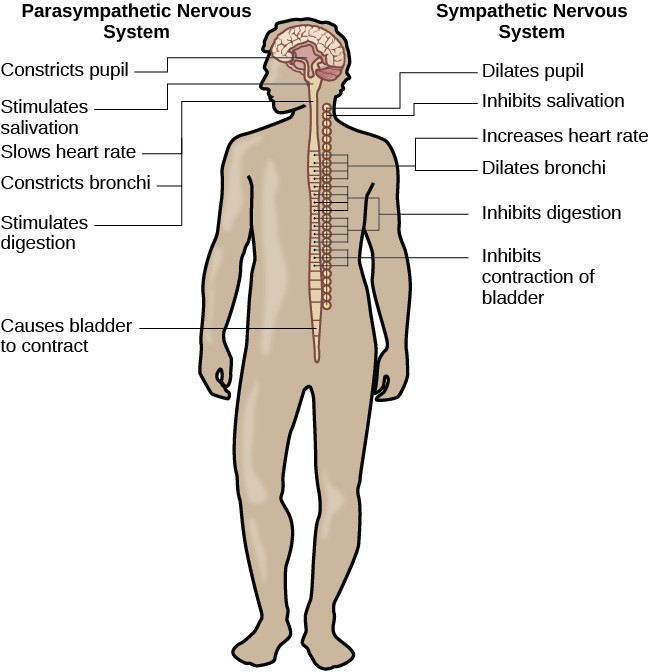
Figure 3.14 The sympathetic and parasympathetic divisions of the autonomic nervous system have the opposite effects on various systems.
The sympathetic nervous system is activated when we are faced with stressful or high-arousal situations. The activity of this system was adaptive for our ancestors, increasing their chances of survival. This constellation of physiological changes, known as the fight or flight response, allows the body access to energy reserves and heightened sensory capacity so that you might fight off a threat or run away to safety.
While it is clear that such a response would be critical for survival for our ancestors, who lived in a world full of real physical threats, many of the high-arousal situations we face in the modern world are more psychological in nature. For example, think about how you feel when you have to stand up and give a presentation in front of a roomful of people, or right before taking a big test. You are in no real physical danger in those situations, and yet you have evolved to respond to any perceived threat with the fight or flight response. This kind of response is not nearly as adaptive in the modern world; in fact, we suffer negative health consequences when faced constantly with psychological threats that we can neither fight nor flee.
Once the threat has been resolved, the parasympathetic nervous system takes over and returns bodily functions to a relaxed state. These processes are associated with activation of the parasympathetic nervous system.
The Brain and Spinal Cord
Learning Objectives:
- Explain the functions of the spinal cord
- Identify the hemispheres and lobes of the brain
- Describe the types of techniques available to clinicians and researchers to image or scan the brain
The brain is a remarkably complex organ comprised of billions of interconnected neurons and glia. It is a bilateral, or two-sided, structure that can be separated into distinct lobes. Each lobe is associated with certain types of functions, but, ultimately, all of the areas of the brain interact with one another to provide the foundation for our thoughts and behaviors. In this section, we discuss the overall organization of the brain and the functions associated with different brain areas, beginning with what can be seen as an extension of the brain, the spinal cord.
THE SPINAL CORD
It can be said that the spinal cord is what connects the brain to the outside world. Because of it, the brain can act. The spinal cord is like a relay station, but a very smart one. It not only routes messages to and from the brain, but it also has its own system of automatic processes, called reflexes.
The top of the spinal cord merges with the brain stem, where the basic processes of life are controlled, such as breathing and digestion. In the opposite direction, the spinal cord ends just below the ribs—contrary to what we might expect, it does not extend all the way to the base of the spine. The spinal cord is functionally organized in 30 segments, corresponding with the vertebrae. Each segment is connected to a specific part of the body through the peripheral nervous system. Nerves branch out from the spine at each vertebra. Sensory nerves bring messages in; motor nerves send messages out to the muscles and organs. Messages travel to and from the brain through every segment.
Some sensory messages are immediately acted on by the spinal cord, without any input from the brain. Withdrawal from heat and knee jerk are two examples. When a sensory message meets certain parameters, the spinal cord initiates an automatic reflex. The signal passes from the sensory nerve to a simple processing center, which initiates a motor command. Seconds are saved, because messages don’t have to go the brain, be processed, and get sent back. In matters of survival, the spinal reflexes allow the body to react extraordinarily fast.
The spinal cord is protected by bony vertebrae and cushioned in cerebrospinal fluid, but injuries still occur. When the spinal cord is damaged in a particular segment, all lower segments are cut off from the brain, causing paralysis. Therefore, the lower on the spine damage is, the fewer functions an injured individual loses.
THE TWO HEMISPHERES
The surface of the brain, known as the cerebral cortex, is very uneven, characterized by a distinctive pattern of folds or bumps, known as gyri (singular: gyrus), and grooves, known as sulci (singular: sulcus), shown in Figure 3.15. These gyri and sulci form important landmarks that allow us to separate the brain into functional centers. The most prominent sulcus, known as the longitudinal fissure, is the deep groove that separates the brain into two halves or hemispheres: the left hemisphere and the right hemisphere.
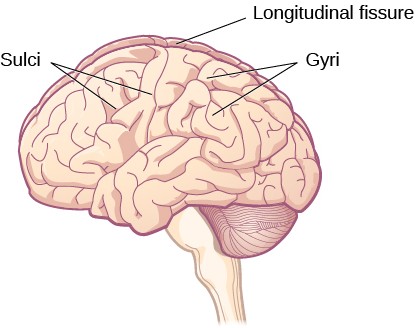
Figure 3.15 The surface of the brain is covered with gyri and sulci. A deep sulcus is called a fissure, such as the longitudinal fissure that divides the brain into left and right hemispheres.
There is evidence of some specialization of function—referred to as lateralization—in each hemisphere, mainly regarding differences in language ability. Beyond that, however, the differences that have been found have been minor. What we do know is that the left hemisphere controls the right half of the body, and the right hemisphere controls the left half of the body.
The two hemispheres are connected by a thick band of neural fibers known as the corpus callosum, consisting of about 200 million axons. The corpus callosum allows the two hemispheres to communicate with each other and allows for information being processed on one side of the brain to be shared with the other side.
Normally, we are not aware of the different roles that our two hemispheres play in day-to-day functions, but there are people who come to know the capabilities and functions of their two hemispheres quite well. In some cases of severe epilepsy, doctors elect to sever the corpus callosum as a means of controlling the spread of seizures (Figure 3.16). While this is an effective treatment option, it results in individuals who have split brains. After surgery, these split-brain patients show a variety of interesting behaviors. For instance, a split-brain patient is unable to name a picture that is shown in the patient’s left visual field because the information is only available in the largely nonverbal right hemisphere. However, they are able to recreate the picture with their left hand, which is also controlled by the right hemisphere. When the more verbal left hemisphere sees the picture that the hand drew, the patient is able to name it (assuming the left hemisphere can interpret what was drawn by the left hand).
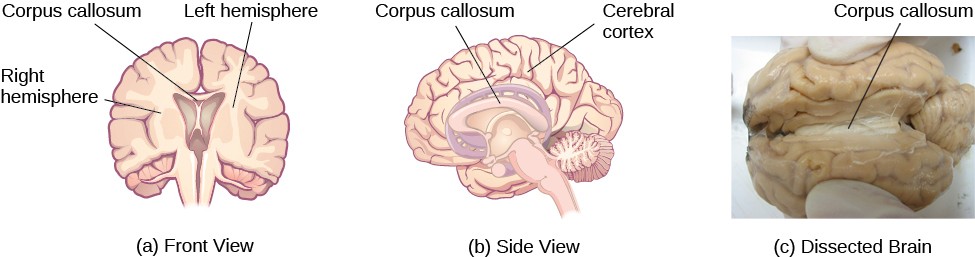
Figure 3.16 (a, b) The corpus callosum connects the left and right hemispheres of the brain. (c) A scientist spreads this dissected sheep brain apart to show the corpus callosum between the hemispheres.
FOREBRAIN STRUCTURES
The two hemispheres of the cerebral cortex are part of the forebrain (Figure3.17), which is the largest part of the brain. The forebrain contains the cerebral cortex and a number of other structures that lie beneath the cortex (called subcortical structures): thalamus, hypothalamus, pituitary gland, and the limbic system (collection of structures). The cerebral cortex, which is the outer surface of the brain, is associated with higher level processes such as consciousness, thought, emotion, reasoning, language, and memory. Each cerebral hemisphere can be subdivided into four lobes, each associated with different functions.
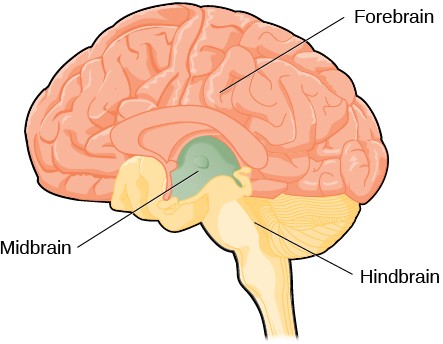
Figure 3.17 The brain and its parts can be divided into three main categories: the forebrain, midbrain, and hindbrain.
Lobes of the Brain
The four lobes of the brain are the frontal, parietal, temporal, and occipital lobes (Figure3.18). The frontal lobe is located in the forward part of the brain, extending back to a fissure known as the central sulcus. The frontal lobe is involved in reasoning, motor control, emotion, and language. It contains the motor cortex, which is involved in planning and coordinating movement; the prefrontal cortex, which is responsible for higher-level cognitive functioning; and Broca’s area, which is essential for language production.
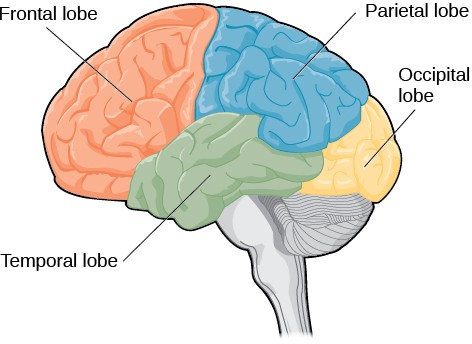
Figure 3.18 The lobes of the brain are shown.
People who suffer damage to Broca’s area have great difficulty producing language of any form (Figure 3.18).
Probably the most famous case of frontal lobe damage is that of a man by the name of Phineas Gage. On September 13, 1848, Gage (age 25) was working as a railroad foreman in Vermont. He and his crew were using an iron rod to tamp explosives down into a blasting hole to remove rock along the railway’s path. Unfortunately, the iron rod created a spark and caused the rod to explode out of the blasting hole, into Gage’s face, and through his skull (Figure 3.19). Although lying in a pool of his own blood with brain matter emerging from his head, Gage was conscious and able to get up, walk, and speak. But in the months following his accident, people noticed that his personality had changed. Many of his friends described him as no longer being himself. Before the accident, it was said that Gage was a well-mannered, soft-spoken man, but he began to behave in odd and inappropriate ways after the accident. Such changes in personality would be consistent with loss of impulse control—a frontal lobe function.
Beyond the damage to the frontal lobe itself, subsequent investigations into the rod’s path also identified probable damage to pathways between the frontal lobe and other brain structures, including the limbic system. With connections between the planning functions of the frontal lobe and the emotional processes of the limbic system severed, Gage had difficulty controlling his emotional impulses.
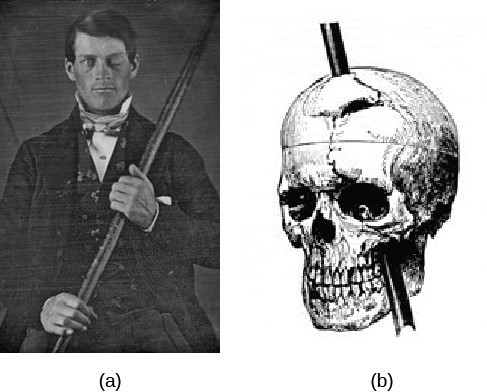
Figure 3.19 (a) Phineas Gage holds the iron rod that penetrated his skull in an 1848 railroad construction accident. (b) Gage’s prefrontal cortex was severely damaged in the left hemisphere. The rod entered Gage’s face on the left side, passed behind his eye, and exited through the top of his skull, before landing about 80 feet away.
The brain’s parietal lobe is located immediately behind the frontal lobe, and is involved in processing information from the body’s senses. It contains the somatosensory cortex, which is essential for processing sensory information from across the body, such as touch, temperature, and pain. The somatosensory cortex is organized topographically, which means that spatial relationships that exist in the body are maintained on the surface of the somatosensory cortex (Figure 3.20). For example, the portion of the cortex that processes sensory information from the hand is adjacent to the portion that processes information from the wrist.
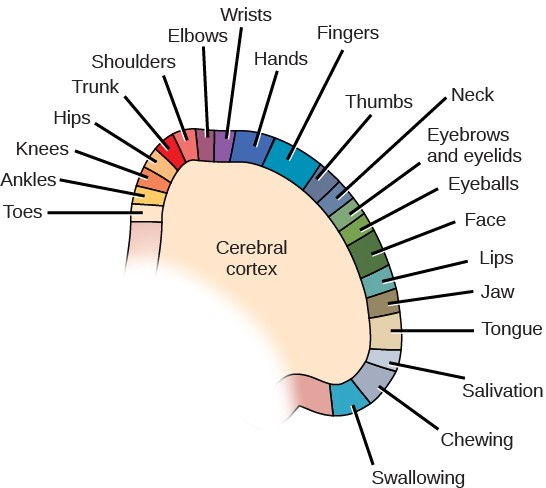
Figure 3.20 Spatial relationships in the body are mirrored in the organization of the somatosensory cortex.
The temporal lobe is located on the side of the head (temporal means “near the temples”), and is associated with hearing, memory, emotion, and some aspects of language. The auditory cortex, the main area responsible for processing auditory information, is located within the temporal lobe. Wernicke’s area, important for speech comprehension, is also located here. Whereas individuals with damage to Broca’s area have difficulty producing language, those with damage to Wernicke’s area can produce sensible language, but they are unable to understand it (Figure3.21).
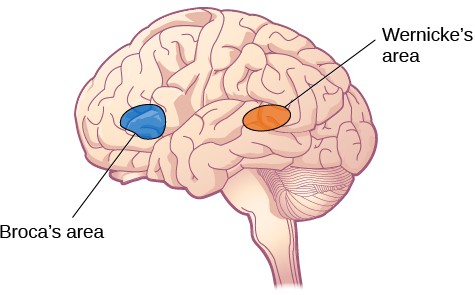
Figure 3.21 Damage to either Broca’s area or Wernicke’s area can result in language deficits. The types of deficits are very different, however, depending on which area is affected.
The occipital lobe is located at the very back of the brain, and contains the primary visual cortex, which is responsible for interpreting incoming visual information. The occipital cortex is organized retinotopically, which means there is a close relationship between the position of an object in a person’s visual field and the position of that object’s representation on the cortex. You will learn much more about how visual information is processed in the occipital lobe when you study sensation and perception.
Other Areas of the Forebrain
Other areas of the forebrain, located beneath the cerebral cortex, include the thalamus and the limbic system. The thalamus is a sensory relay for the brain. All of our senses, with the exception of smell, are routed through the thalamus before being directed to other areas of the brain for processing (Figure 3.22).
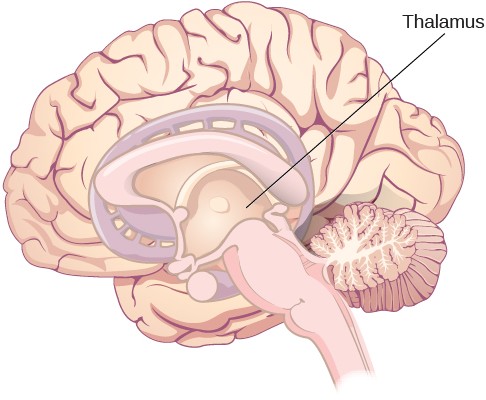
Figure 3.22 The thalamus serves as the relay center of the brain where most senses are routed for processing.
The limbic system is involved in processing both emotion and memory. Interestingly, the sense of smell projects directly to the limbic system; therefore, not surprisingly, smell can evoke emotional responses in ways that other sensory modalities cannot. The limbic system is made up of a number of different structures, but three of the most important are the hippocampus, the amygdala, and the hypothalamus (Figure 3.23). The hippocampus is an essential structure for learning and memory. The amygdala is involved in our experience of emotion and in tying emotional meaning to our memories. The hypothalamus regulates a number of homeostatic processes, including the regulation of body temperature, appetite, and blood pressure. The hypothalamus also serves as an interface between the nervous system and the endocrine system and in the regulation of sexual motivation and behavior.

Figure 3.23 The limbic system is involved in mediating emotional response and memory.
MIDBRAIN AND HINDBRAIN STRUCTURES
The midbrain is comprised of structures located deep within the brain, between the forebrain and the hindbrain. The reticular formation is centered in the midbrain, but it actually extends up into the forebrain and down into the hindbrain. The reticular formation is important in regulating the sleep/wake cycle, arousal, alertness, and motor activity.
The hindbrain is located at the back of the head and looks like an extension of the spinal cord. It contains the medulla, pons, and cerebellum (Figure 3.25). The medulla controls the automatic processes of the autonomic nervous system, such as breathing, blood pressure, and heart rate. The word pons literally means “bridge,” and as the name suggests, the pons serves to connect the brain and spinal cord. It also is involved in regulating brain activity during sleep. The medulla, pons, and midbrain together are known as the brainstem.
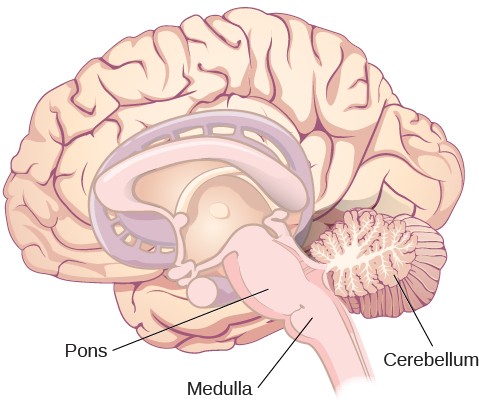
Figure 3.25 The pons, medulla, and cerebellum make up the hindbrain.
The cerebellum (Latin for “little brain”) receives messages from muscles, tendons, joints, and structures in our ear to control balance, coordination, movement, and motor skills. The cerebellum is also thought to be an important area for processing some types of memories. In particular, procedural memory, or memory involved in learning and remembering how to perform tasks, is thought to be associated with the cerebellum.
The Endocrine System
Learning Objectives
- Identify the major glands of the endocrine system
- Identify the hormones secreted by each gland
- Describe each hormone’s role in regulating bodily functions
The endocrine system consists of a series of glands that produce chemical substances known as hormones (Figure3.30). Like neurotransmitters, hormones are chemical messengers that must bind to a receptor in order to send their signal. However, unlike neurotransmitters, which are released in close proximity to cells with their receptors, hormones are secreted into the bloodstream and travel throughout the body, affecting any cells that contain receptors for them. Thus, whereas neurotransmitters’ effects are localized, the effects of hormones are widespread. Also, hormones are slower to take effect, and tend to be longer lasting.
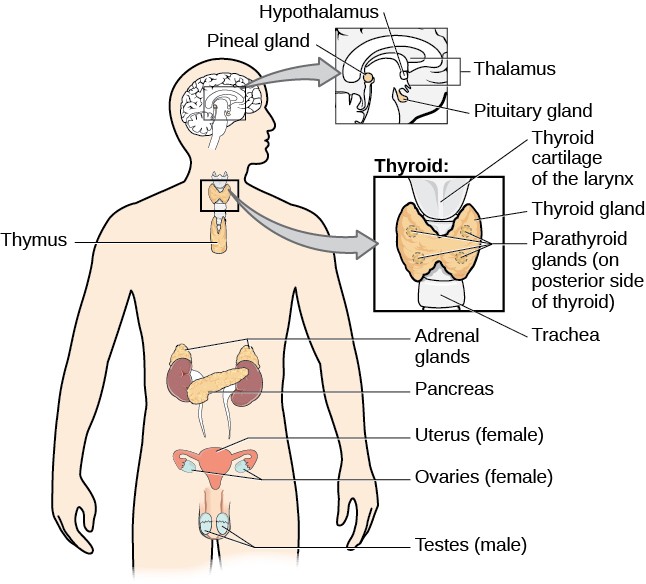
Figure 3.30 The major glands of the endocrine system are shown.
Hormones are involved in regulating all sorts of bodily functions, and they are ultimately controlled through interactions between the hypothalamus (in the central nervous system) and the pituitary gland (in the endocrine system). Imbalances in hormones are related to a number of disorders. This section explores some of the major glands that make up the endocrine system and the hormones secreted by these glands.
MAJOR GLANDS
The pituitary gland descends from the hypothalamus at the base of the brain, and acts in close association with it. The pituitary is often referred to as the “master gland” because its messenger hormones control all the other glands in the endocrine system, although it mostly carries out instructions from the hypothalamus. In addition to messenger hormones, the pituitary also secretes growth hormone, endorphins for pain relief, and a number of key hormones that regulate fluid levels in the body.
Located in the neck, the thyroid gland releases hormones that regulate growth, metabolism, and appetite. In hyperthyroidism, or Grave’s disease, the thyroid secretes too much of the hormone thyroxine, causing agitation, bulging eyes, and weight loss. In hypothyroidism, reduced hormone levels cause sufferers to experience tiredness, and they often complain of feeling cold. Fortunately, thyroid disorders are often treatable with medications that help reestablish a balance in the hormones secreted by the thyroid.
The adrenal glands sit atop our kidneys and secrete hormones involved in the stress response, such as epinephrine (adrenaline) and norepinephrine (noradrenaline). The pancreas is an internal organ that secretes hormones that regulate blood sugar levels: insulin and glucagon. These pancreatic hormones are essential for maintaining stable levels of blood sugar throughout the day by lowering blood glucose levels (insulin) or raising them (glucagon). People who suffer from diabetes do not produce enough insulin; therefore, they must take medications that stimulate or replace insulin production, and they must closely control the amount of sugars and carbohydrates they consume.
The gonads secrete sexual hormones, which are important in reproduction, and mediate both sexual motivation and behavior. The female gonads are the ovaries; the male gonads are the testes. Ovaries secrete estrogens and progesterone, and the testes secrete androgens, such as testosterone.
What is Stress
Learning Objectives
- Differentiate between stimulus-based and response-based definitions of stress
- Define stress as a process
- Differentiate between good stress and bad stress
- Understand the physiological basis of stress and describe the general adaptation syndrome
The term stress as it relates to the human condition first emerged in scientific literature in the 1930s, but it did not enter the popular vernacular until the 1970s (Lyon, 2012). Today, we often use the term loosely in describing a variety of unpleasant feeling states; for example, we often say we are stressed out when we feel frustrated, angry, conflicted, overwhelmed, or fatigued. Despite the widespread use of the term, stress is a fairly vague concept that is difficult to define with precision.
Researchers have had a difficult time agreeing on an acceptable definition of stress. Some have conceptualized stress as a demanding or threatening event or situation (e.g., a high-stress job, overcrowding, and long commutes to work). Such conceptualizations are known as stimulus-based definitions because they characterize stress as a stimulus that causes certain reactions. Stimulus-based definitions of stress are problematic, however, because they fail to recognize that people differ in how they view and react to challenging life events and situations.
Others have conceptualized stress in ways that emphasize the physiological responses that occur when faced with demanding or threatening situations (e.g., increased arousal). These conceptualizations are referred to as response-based definitions because they describe stress as a response to environmental conditions. Neither stimulus- based nor response-based definitions provide a complete definition of stress. Many of the physiological reactions that occur when faced with demanding situations (e.g., accelerated heart rate) can also occur in response to things that most people would not consider to be genuinely stressful, such as receiving unanticipated good news: an unexpected promotion or raise.
A useful way to conceptualize stress is to view it as a process whereby an individual perceives and responds to events that he appraises as overwhelming or threatening to his well-being (Lazarus & Folkman, 1984). A critical element of this definition is that it emphasizes the importance of how we appraise—that is, judge—demanding or threatening events (often referred to as stressors); these appraisals, in turn, influence our reactions to such events. Two kinds of appraisals of a stressor are especially important in this regard: primary and secondary appraisals. A primary appraisal involves judgment about the degree of potential harm or threat to well-being that a stressor might entail. A stressor would likely be appraised as a threat if one anticipates that it could lead to some kind of harm, loss, or other negative consequence; conversely, a stressor would likely be appraised as a challenge if one believes that it carries the potential for gain or personal growth. For example, an employee who is promoted to a leadership position would likely perceive the promotion as a much greater threat if she believed the promotion would lead to excessive work demands than if she viewed it as an opportunity to gain new skills and grow professionally.
The perception of a threat triggers a secondary appraisal: judgment of the options available to cope with a stressor, as well as perceptions of how effective such options will be (Lyon, 2012) (Figure14.3). As you may recall from what you learned about self-efficacy, an individual’s belief in his ability to complete a task is important (Bandura, 1994). A threat tends to be viewed as less catastrophic if one believes something can be done about it (Lazarus & Folkman, 1984).

Figure 14.3 When encountering a stressor, a person judges its potential threat (primary appraisal) and then determines if effective options are available to manage the situation. Stress is likely to result if a stressor is perceived as extremely threatening or threatening with few or no effective coping options available.
To be sure, some stressors are inherently more stressful than others in that they are more threatening and leave less potential for variation in cognitive appraisals (e.g., objective threats to one’s health or safety). Nevertheless, appraisal will still play a role in augmenting or diminishing our reactions to such events (Everly & Lating, 2002).
If a person appraises an event as harmful and believes that the demands imposed by the event exceed the available resources to manage or adapt to it, the person will subjectively experience a state of stress. In contrast, if one does not appraise the same event as harmful or threatening, she is unlikely to experience stress. According to this definition, environmental events trigger stress reactions by the way they are interpreted and the meanings they are assigned. In short, stress is largely in the eye of the beholder: it’s not so much what happens to you as it is how you respond (Selye, 1976).
GOOD STRESS?
Although stress carries a negative connotation, at times it may be of some benefit. Stress can motivate us to do things in our best interests, such as study for exams, visit the doctor regularly, exercise, and perform to the best of our ability at work. Indeed, Selye (1974) pointed out that not all stress is harmful.
He argued that stress can sometimes be a positive, motivating force that can improve the quality of our lives. This kind of stress, which Selye called eustress (from the Greek eu = “good”), is a good kind of stress associated with positive feelings, optimal health, and performance. A moderate amount of stress can be beneficial in challenging situations. For example, athletes may be motivated and energized by pregame stress, and students may experience similar beneficial stress before a major exam.
Increasing one’s level of stress will cause performance to change in a predictable way. As shown in Figure 14.4, as stress increases, so do performance and general well-being (eustress); when stress levels reach an optimal level (the highest point of the curve), performance reaches its peak. A person at this stress level is colloquially at the top of his game, meaning he feels fully energized, focused, and can work with minimal effort and maximum efficiency. But when stress exceeds this optimal level, it is no longer a positive force—it becomes excessive and debilitating, or what Selye termed distress (from the Latin dis = “bad”). People who reach this level of stress feel burned out; they are fatigued, exhausted, and their performance begins to decline. If the stress remains excessive, health may begin to erode as well (Everly & Lating, 2002).
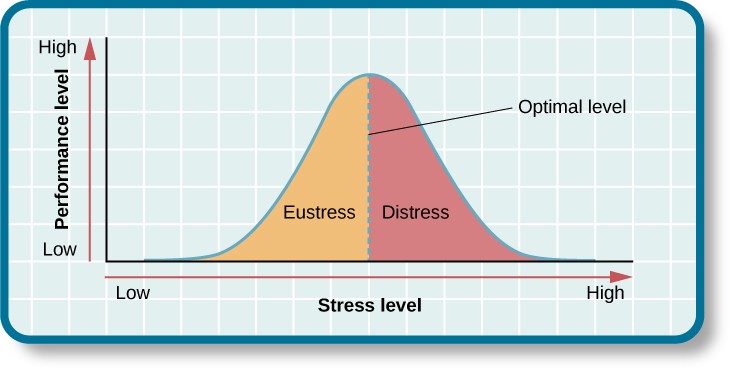
Figure 14.4 As the stress level increases from low to moderate, so does performance (eustress). At the optimal level (the peak of the curve), performance has reached its peak. If stress exceeds the optimal level, it will reach the distress region, where it will become excessive and debilitating, and performance will decline (Everly & Lating, 2002).
THE PREVALENCE OF STRESS
Stress is everywhere and, as shown in Figure 14.5, it has been on the rise over the last several years. Each of us is acquainted with stress—some are more familiar than others. In many ways, stress feels like a load you just can’t carry—a feeling you experience.
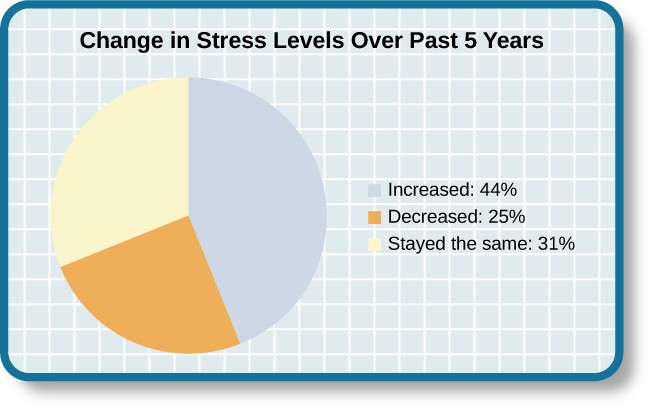
Figure 14.5 Nearly half of U.S. adults indicated that their stress levels have increased over the last five years (Neelakantan, 2013).
Stress is an experience that evokes a variety of responses, including those that are physiological (e.g., accelerated heart rate, headaches, or gastrointestinal problems), cognitive (e.g., difficulty concentrating or making decisions), and behavioral (e.g., drinking alcohol, smoking, or taking actions directed at eliminating the cause of the stress). Although stress can be positive at times, it can have deleterious health implications, contributing to the onset and progression of a variety of physical illnesses and diseases (Cohen & Herbert, 1996).
THE PHYSIOLOGICAL BASIS OF STRESS
What goes on inside our bodies when we experience stress? The physiological mechanisms of stress are extremely complex, but they generally involve the work of two systems—the sympathetic nervous system and the hypothalamic-pituitary-adrenal (HPA) axis. When a person first perceives something as stressful (Selye’s alarm reaction), the sympathetic nervous system triggers arousal via the release of adrenaline from the adrenal glands. Release of these hormones activates the fight-or-flight responses to stress, such as accelerated heart rate and respiration. At the same time, the HPA axis, which is primarily endocrine in nature, becomes especially active, although it works much more slowly than the sympathetic nervous system. In response to stress, the hypothalamus (one of the limbic structures in the brain) releases corticotrophin-releasing factor, a hormone that causes the pituitary gland to release adrenocorticotropic hormone (ACTH) (Figure 14.11). The ACTH then activates the adrenal glands to secrete a number of hormones into the bloodstream; an important one is cortisol, which can affect virtually every organ within the body. Cortisol is commonly known as a stress hormone and helps provide that boost of energy when we first encounter a stressor, preparing us to run away or fight. However, sustained elevated levels of cortisol weaken the immune system.
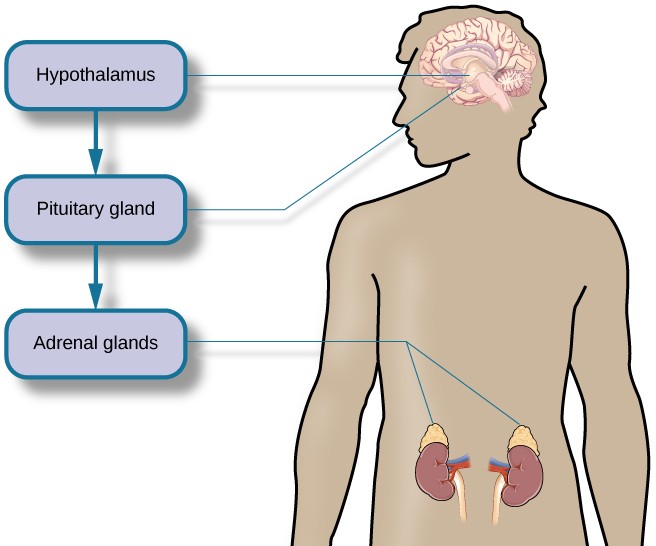
Figure 14.11 This diagram shows the functioning of the hypothalamic-pituitary-adrenal (HPA) axis. The hypothalamus activates the pituitary gland, which in turn activates the adrenal glands, increasing their secretion of cortisol.
In short bursts, this process can have some favorable effects, such as providing extra energy, improving immune system functioning temporarily, and decreasing pain sensitivity. However, extended release of cortisol—as would happen with prolonged or chronic stress—often comes at a high price. High levels of cortisol have been shown to produce a number of harmful effects. For example, increases in cortisol can significantly weaken our immune system (Glaser & Kiecolt-Glaser, 2005), and high levels are frequently observed among depressed individuals (Geoffroy, Hertzman, Li, & Power, 2013). In summary, a stressful event causes a variety of physiological reactions that activate the adrenal glands, which in turn release epinephrine, norepinephrine, and cortisol. These hormones affect a number of bodily processes in ways that prepare the stressed person to take direct action, but also in ways that may heighten the potential for illness.
When stress is extreme or chronic, it can have profoundly negative consequences. For example, stress often contributes to the development of certain psychological disorders, including post-traumatic stress disorder, major depressive disorder, and other serious psychiatric conditions. Additionally, we noted earlier that stress is linked to the development and progression of a variety of physical illnesses and diseases.
Stress and Illness
Learning Objectives
- Explain the nature of psychophysiological disorders
- Describe the immune system and how stress impacts its functioning
- Describe how stress and emotional factors can lead to the development and exacerbation of cardiovascular disorders, asthma, and tension headaches
In this section, we will discuss stress and illness. As stress researcher Robert Sapolsky (1998) describes,
stress-related disease emerges, predominantly, out of the fact that we so often activate a physiological system that has evolved for responding to acute physical emergencies, but we turn it on for months on end, worrying about mortgages, relationships, and promotions. (p. 6)
The stress response, as noted earlier, consists of a coordinated but complex system of physiological reactions that are called upon as needed. These reactions are beneficial at times because they prepare us to deal with potentially dangerous or threatening situations. However, health is affected when physiological reactions are sustained, as can happen in response to ongoing stress.
PSYCHOPHYSIOLOGICAL DISORDERS
If the reactions that compose the stress response are chronic or if they frequently exceed normal ranges, they can lead to cumulative wear and tear on the body, in much the same way that running your air conditioner on full blast all summer will eventually cause wear and tear on it. For example, the high blood pressure that a person under considerable job strain experiences might eventually take a toll on his heart and set the stage for a heart attack or heart failure. Also, someone exposed to high levels of the stress hormone cortisol might become vulnerable to infection or disease because of weakened immune system functioning (McEwen, 1998).
Physical disorders or diseases whose symptoms are brought about or worsened by stress and emotional factors are called psychophysiological disorders. The physical symptoms of psychophysiological disorders are real and they can be produced or exacerbated by psychological factors (hence the psycho and physiological in psychophysiological). A list of frequently encountered psychophysiological disorders is provided in Table14.3.
|
Table 14.3 Types of Psychophysiological Disorders (adapted from Everly & Lating, 2002) |
|
|
Type of Psychophysiological Disorder |
Examples |
|
Cardiovascular |
hypertension, coronary heart disease |
|
Gastrointestinal |
irritable bowel syndrome |
|
Respiratory |
asthma, allergy |
|
Musculoskeletal |
low back pain, tension headaches |
|
Skin |
acne, eczema, psoriasis |
STRESS AND THE IMMUNE SYSTEM
In a sense, the immune system is the body’s surveillance system. It consists of a variety of structures, cells, and mechanisms that serve to protect the body from invading toxins and microorganisms that can harm or damage the body’s tissues and organs. When the immune system is working as it should, it keeps us healthy and disease free by eliminating bacteria, viruses, and other foreign substances that have entered the body (Everly & Lating, 2002).
Stressors and Immune Function
The question of whether stress and negative emotional states can influence immune function has captivated researchers for over three decades, and discoveries made over that time have dramatically changed the face of health psychology (Kiecolt-Glaser, 2009). Psychoneuroimmunology is the field that studies how psychological factors such as stress influence the immune system and immune functioning. To a large extent, this field evolved from the discovery that there is a connection between the central nervous system and the immune system.
Some of the most compelling evidence for a connection between the brain and the immune system comes from studies in which researchers demonstrated that immune responses in animals could be classically conditioned (Everly & Lating, 2002). For example, Ader and Cohen (1975) paired flavored water (the conditioned stimulus) with the presentation of an immunosuppressive drug (the unconditioned stimulus), causing sickness (an unconditioned response). Not surprisingly, rats exposed to this pairing developed a conditioned aversion to the flavored water. However, the taste of the water itself later produced immunosuppression (a conditioned response), indicating that the immune system itself had been conditioned. Thus, if classical conditioning can alter immunity, other psychological factors should be capable of altering it as well.
Summary
Cells of the Nervous System
Glia and neurons are the two cell types that make up the nervous system. While glia generally play supporting roles, the communication between neurons is fundamental to all of the functions associated with the nervous system. Neuronal communication is made possible by the neuron’s specialized structures. The soma contains the cell nucleus, and the dendrites extend from the soma in tree-like branches. The axon is another major extension of the cell body; axons are often covered by a myelin sheath, which increases the speed of transmission of neural impulses. At the end of the axon are terminal buttons that contain synaptic vesicles filled with neurotransmitters.
Neuronal communication is an electrochemical event. The dendrites contain receptors for neurotransmitters released by nearby neurons. If the signals received from other neurons are sufficiently strong, an action potential will travel down the length of the axon to the terminal buttons, resulting in the release of neurotransmitters into the synapse. Action potentials operate on the all-or-none principle and involve the movement of Na+ and K+ across the neuronal membrane.
Different neurotransmitters are associated with different functions. Often, psychological disorders involve imbalances in a given neurotransmitter system. Therefore, psychotropic drugs are prescribed in an attempt to bring the neurotransmitters back into balance. Drugs can act either as agonists or as antagonists for a given neurotransmitter system.
Parts of the Nervous System
The brain and spinal cord make up the central nervous system. The peripheral nervous system is comprised of the somatic and autonomic nervous systems. The somatic nervous system transmits sensory and motor signals to and from the central nervous system. The autonomic nervous system controls the function of our organs and glands, and can be divided into the sympathetic and parasympathetic divisions. Sympathetic activation prepares us for fight or flight, while parasympathetic activation is associated with normal functioning under relaxed conditions.
The Brain and Spinal Cord
The brain consists of two hemispheres, each controlling the opposite side of the body. Each hemisphere can be subdivided into different lobes: frontal, parietal, temporal, and occipital. In addition to the lobes of the cerebral cortex, the forebrain includes the thalamus (sensory relay) and limbic system (emotion and memory circuit). The midbrain contains the reticular formation, which is important for sleep and arousal, as well as the substantia nigra and ventral tegmental area. These structures are important for movement, reward, and addictive processes. The hindbrain contains the structures of the brainstem (medulla, pons, and midbrain), which control automatic functions like breathing and blood pressure. The hindbrain also contains the cerebellum, which helps coordinate movement and certain types of memories.
Individuals with brain damage have been studied extensively to provide information about the role of different areas of the brain, and recent advances in technology allow us to glean similar information by imaging brain structure and function. These techniques include CT, PET, MRI, fMRI, and EEG.
The Endocrine System
The glands of the endocrine system secrete hormones to regulate normal body functions. The hypothalamus serves as the interface between the nervous system and the endocrine system, and it controls the secretions of the pituitary. The pituitary serves as the master gland, controlling the secretions of all other glands. The thyroid secretes thyroxine, which is important for basic metabolic processes and growth; the adrenal glands secrete hormones involved in the stress response; the pancreas secretes hormones that regulate blood sugar levels; and the ovaries and testes produce sex hormones that regulate sexual motivation and behavior.