
Chapter 4: States of Consciousness
Introduction
Our lives involve regular, dramatic changes in the degree to which we are aware of our surroundings and our internal states. While awake, we feel alert and aware of the many important things going on around us. Our experiences change dramatically while we are in deep sleep and once again when we are dreaming.
This chapter will discuss states of consciousness with a particular emphasis on sleep. The different stages of sleep will be identified, and sleep disorders will be described. The chapter will close with discussions of altered states of consciousness produced by psychoactive drugs, hypnosis, and meditation.
What is Consciousness
Learning Objectives
By the end of this section, you will be able to:
- Understand what is meant by consciousness
- Explain how circadian rhythms are involved in regulating the sleep-wake cycle, and how circadian cycles can be disrupted
- Discuss the concept of sleep debt
Consciousness describes our awareness of internal and external stimuli. Awareness of internal stimuli includes feeling pain, hunger, thirst, sleepiness, and being aware of our thoughts and emotions. Awareness of external stimuli includes seeing the light from the sun, feeling the warmth of a room, and hearing the voice of a friend.
We experience different states of consciousness and different levels of awareness on a regular basis. We might even describe consciousness as a continuum that ranges from full awareness to a deep sleep. Sleep is a state marked by relatively low levels of physical activity and reduced sensory awareness that is distinct from periods of rest that occur during wakefulness. Wakefulness is characterized by high levels of sensory awareness, thought, and behavior. In between these extremes are states of consciousness related to daydreaming, intoxication as a result of alcohol or other drug use, meditative states, hypnotic states, and altered states of consciousness following sleep deprivation. We might also experience unconscious states of being via drug-induced anesthesia for medical purposes. Often, we are not completely aware of our surroundings, even when we are fully awake. For instance, have you ever daydreamed while driving home from work or school without really thinking about the drive itself? You were capable of engaging in the all of the complex tasks involved with operating a motor vehicle even though you were not aware of doing so. Many of these processes, like much of psychological behavior, are rooted in our biology.
BIOLOGICAL RHYTHMS
Biological rhythms are internal rhythms of biological activity. A woman’s menstrual cycle is an example of a biological rhythm—a recurring, cyclical pattern of bodily changes. One complete menstrual cycle takes about 28 days—a lunar month—but many biological cycles are much shorter. For example, body temperature fluctuates cyclically over a 24-hour period (Figure 4.2). Alertness is associated with higher body temperatures, and sleepiness with lower body temperatures.
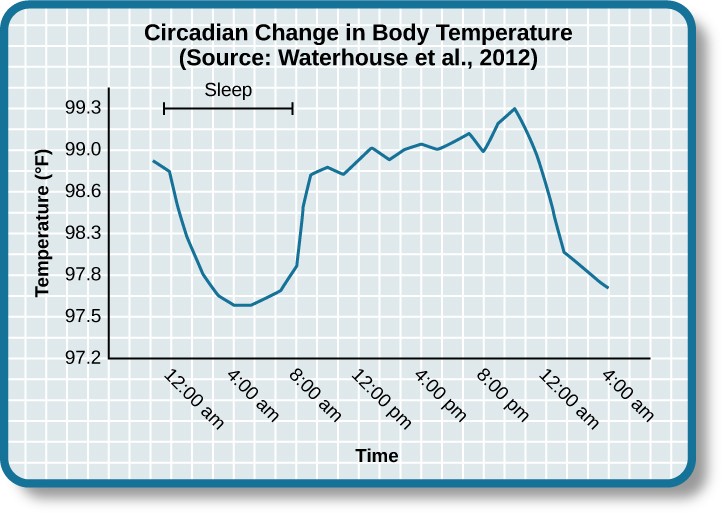
Figure 4.2 This chart illustrates the circadian change in body temperature over 28 hours in a group of eight young men. Body temperature rises throughout the waking day, peaking in the afternoon, and falls during sleep with the lowest point occurring during the very early morning hours.
This pattern of temperature fluctuation, which repeats every day, is one example of a circadian rhythm. A circadian rhythm is a biological rhythm that takes place over a period of about 24 hours. Our sleep-wake cycle, which is linked to our environment’s natural light-dark cycle, is perhaps the most obvious example of a circadian rhythm, but we also have daily fluctuations in heart rate, blood pressure, blood sugar, and body temperature. Some circadian rhythms play a role in changes in our state of consciousness.
If we have biological rhythms, then is there some sort of biological clock? In the brain, the hypothalamus, which lies above the pituitary gland, is a main center of homeostasis. Homeostasis is the tendency to maintain a balance, or optimal level, within a biological system.
The brain’s clock mechanism is located in an area of the hypothalamus known as the suprachiasmatic nucleus (SCN). The axons of light-sensitive neurons in the retina provide information to the SCN based on the amount of light present, allowing this internal clock to be synchronized with the outside world (Klein, Moore, & Reppert, 1991; Welsh, Takahashi, & Kay, 2010) (Figure4.3).
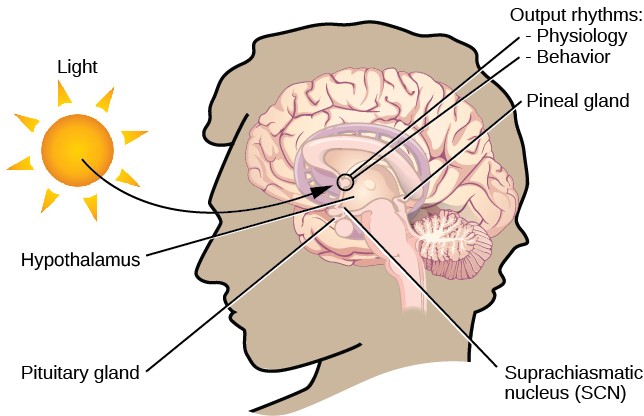
Figure 4.3 The suprachiasmatic nucleus (SCN) serves as the brain’s clock mechanism. The clock sets itself with light information received through projections from the retina.
Disruptions of Normal Sleep
Whether lark, owl, or somewhere in between, there are situations in which a person’s circadian clock gets out of synchrony with the external environment. One way that this happens involves traveling across multiple time zones. When we do this, we often experience jet lag. Jet lag is a collection of symptoms that results from the mismatch between our internal circadian cycles and our environment. These symptoms include fatigue, sluggishness, irritability, and insomnia (i.e., a consistent difficulty in falling or staying asleep for at least three nights a week over a month’s time) (Roth, 2007).
While disruptions in circadian rhythms can have negative consequences, there are things we can do to help us realign our biological clocks with the external environment. Some of these approaches, such as using a bright light as shown in Figure 4.4, have been shown to alleviate some of the problems experienced by individuals suffering from jet lag or from the consequences of rotating shift work. Because the biological clock is driven by light, exposure to bright light during working shifts and dark exposure when not working can help combat insomnia and symptoms of anxiety and depression (Huang, Tsai, Chen, & Hsu, 2013).

Figure 4.4 Devices like this are designed to provide exposure to bright light to help people maintain a regular circadian cycle. They can be helpful for people working night shifts or for people affected by seasonal variations in light.
Insufficient Sleep
When people have difficulty getting sleep due to their work or the demands of day-to-day life, they accumulate a sleep debt. A person with a sleep debt does not get sufficient sleep on a chronic basis. The consequences of sleep debt include decreased levels of alertness and mental efficiency. Interestingly, since the advent of electric light, the amount of sleep that people get has declined. While we certainly welcome the convenience of having the darkness lit up, we also suffer the consequences of reduced amounts of sleep because we are more active during the nighttime hours than our ancestors were. As a result, many of us sleep less than 7–8 hours a night and accrue a sleep debt. While there is tremendous variation in any given individual’s sleep needs, the National Sleep Foundation (n.d.) cites research to estimate that newborns require the most sleep (between 12 and 18 hours a night) and that this amount declines to just 7–9 hours by the time we are adults. Table 4.1 shows recommended amounts of sleep at different ages.
|
Table 4.1 Sleep Needs at Different Ages |
|
|
Age |
Nightly Sleep Needs |
|
0–3 months |
12–18 hours |
|
3 months–1 year |
14–15 hours |
|
1–3 years |
12–14 hours |
|
3–5 years |
11–13 hours |
|
5–10 years |
10–11 hours |
|
10–18 years |
8–10 hours |
|
18 and older |
7–9 hours |
Sleep debt and sleep deprivation have significant negative psychological and physiological consequences Figure 4.5. As mentioned earlier, lack of sleep can result in decreased mental alertness and cognitive function. In addition, sleep deprivation often results in depression-like symptoms. These effects can occur as a function of accumulated sleep debt or in response to more acute periods of sleep deprivation. It may surprise you to know that sleep deprivation is associated with obesity, increased blood pressure, increased levels of stress hormones, and reduced immune functioning (Banks & Dinges, 2007).
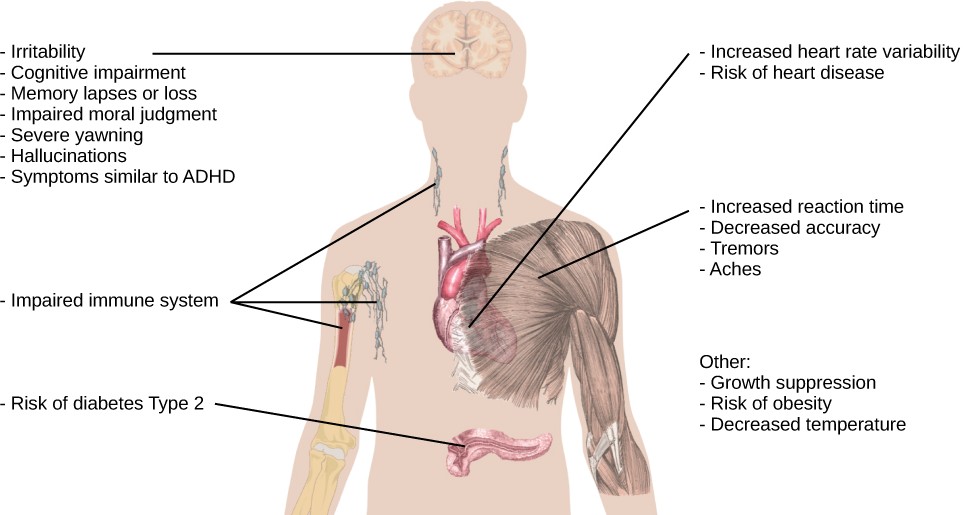
Figure 4.5 This figure illustrates some of the negative consequences of sleep deprivation. While cognitive deficits may be the most obvious, many body systems are negatively impacted by lack of sleep. (credit: modification of work by Mikael Häggström)
The amount of sleep we get varies across the lifespan. When we are very young, we spend up to 16 hours a day sleeping. As we grow older, we sleep less. In fact, a meta-analysis, which is a study that combines the results of many related studies, conducted within the last decade indicates that by the time we are 65 years old, we average fewer than 7 hours of sleep per day (Ohayon, Carskadon, Guilleminault, & Vitiello, 2004). As the amount of time we sleep varies over our lifespan, presumably the sleep debt would adjust accordingly.
Sleep and Why We Sleep?
Learning Objectives
By the end of this section, you will be able to:
- Describe areas of the brain involved in sleep
- Understand hormone secretions associated with sleep
- Describe several theories aimed at explaining the function of sleep
We spend approximately one-third of our lives sleeping. Given the average life expectancy for U.S. citizens falls between 73 and 79 years old (Singh & Siahpush, 2006), we can expect to spend approximately 25 years of our lives sleeping. Some animals never sleep (e.g., several fish and amphibian species); other animals can go extended periods of time without sleep and without apparent negative consequences (e.g., dolphins); yet some animals (e.g., rats) die after two weeks of sleep deprivation (Siegel, 2008). Why do we devote so much time to sleeping? Is it absolutely essential that we sleep? This section will consider these questions and explore various explanations for why we sleep.
WHAT IS SLEEP?
You have read that sleep is distinguished by low levels of physical activity and reduced sensory awareness. As discussed by Siegel (2008), a definition of sleep must also include mention of the interplay of the circadian and homeostatic mechanisms that regulate sleep. Homeostatic regulation of sleep is evidenced by sleep rebound following sleep deprivation. Sleep rebound refers to the fact that a sleep- deprived individual will tend to take a shorter time to fall asleep during subsequent opportunities for sleep. Sleep is characterized by certain patterns of activity of the brain that can be visualized using electroencephalography (EEG), and different phases of sleep can be differentiated using EEG as well (Figure4.6).
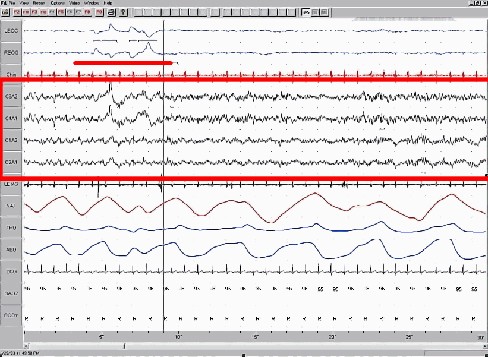
Figure 4.6 This is a segment of a polysonograph (PSG), a recording of several physical variables during sleep. The x-axis shows passage of time in seconds; this record includes 30 seconds of data. The location of the sets of electrode that produced each signal is labeled on the y-axis. The red box encompasses EEG output, and the waveforms are characteristic of a specific stage of sleep. Other curves show other sleep-related data, such as body temperature, muscle activity, and heartbeat.
Sleep is also associated with the secretion and regulation of a number of hormones from several endocrine glands including: melatonin, follicle stimulating hormone (FSH), luteinizing hormone (LH), and growth hormone (National Institutes of Health, n.d.). You have read that the pineal gland releases melatonin during sleep (Figure 4.7). Melatonin is thought to be involved in the regulation of various biological rhythms and the immune system (Hardeland et al., 2006). During sleep, the pituitary gland secretes both FSH and LH which are important in regulating the reproductive system (Christensen et al., 2012; Sofikitis et al., 2008). The pituitary gland also secretes growth hormone, during sleep, which plays a role in physical growth and maturation as well as other metabolic processes (Bartke, Sun, & Longo, 2013).
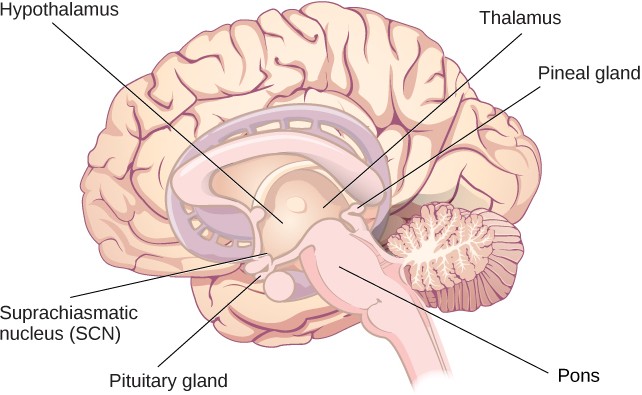
Figure 4.7 The pineal and pituitary glands secrete a number of hormones during sleep.
WHY DO WE SLEEP?
Given the central role that sleep plays in our lives and the number of adverse consequences that have been associated with sleep deprivation, one would think that we would have a clear understanding of why it is that we sleep. Unfortunately, this is not the case; however, several hypotheses have been proposed to explain the function of sleep.
Adaptive Function of Sleep
One popular hypothesis of sleep incorporates the perspective of evolutionary psychology. Evolutionary psychology is a discipline that studies how universal patterns of behavior and cognitive processes have evolved over time as a result of natural selection. Variations and adaptations in cognition and behavior make individuals more or less successful in reproducing and passing their genes to their offspring. One hypothesis from this perspective might argue that sleep is essential to restore resources that are expended during the day. Just as bears hibernate in the winter when resources are scarce, perhaps people sleep at night to reduce their energy expenditures. Another evolutionary hypothesis of sleep holds that our sleep patterns evolved as an adaptive response to predatory risks, which increase in darkness. Thus we sleep in safe areas to reduce the chance of harm. Comparative research indicates, however, that the relationship that exists between predatory risk and sleep is very complex and equivocal.
It is quite possible that sleep serves no single universally adaptive function, and different species have evolved different patterns of sleep in response to their unique evolutionary pressures. While we have discussed the negative outcomes associated with sleep deprivation, it should be pointed out that there are many benefits that are associated with adequate amounts of sleep. A few such benefits listed by the National Sleep Foundation (n.d.) include maintaining healthy weight, lowering stress levels, improving mood, and increasing motor coordination, as well as a number of benefits related to cognition and memory formation.
Cognitive Function of Sleep
Another theory regarding why we sleep involves sleep’s importance for cognitive function and memory formation (Rattenborg, Lesku, Martinez-Gonzalez, & Lima, 2007). Indeed, we know sleep deprivation results in disruptions in cognition and memory deficits (Brown, 2012), leading to impairments in our abilities to maintain attention, make decisions, and recall long-term memories. Moreover, these impairments become more severe as the amount of sleep deprivation increases (Alhola & Polo-Kantola, 2007). Furthermore, slow-wave sleep after learning a new task can improve resultant performance on that task (Huber, Ghilardi, Massimini, & Tononi, 2004) and seems essential for effective memory formation (Stickgold, 2005). Understanding the impact of sleep on cognitive function should help you understand that cramming all night for a test may be not effective and can even prove counterproductive.
Sleep has also been associated with other cognitive benefits. Research indicates that included among these possible benefits are increased capacities for creative thinking (Cai, Mednick, Harrison, Kanady, & Mednick, 2009; Wagner, Gais, Haider, Verleger, & Born, 2004), language learning (Fenn, Nusbaum, & Margoliash, 2003; Gómez, Bootzin, & Nadel, 2006), and inferential judgments (Ellenbogen, Hu, Payne, Titone, & Walker, 2007). It is possible that even the processing of emotional information is influenced by certain aspects of sleep (Walker, 2009).
Substanace Use and Abuse
Learning Objectives
By the end of this section, you will be able to:
- Describe the diagnostic criteria for substance use disorders
- Identify the neurotransmitter systems affected by various categories of drugs
- Describe how different categories of drugs effect behavior and experience
While we all experience altered states of consciousness in the form of sleep on a regular basis, some people use drugs and other substances that result in altered states of consciousness as well. This section will present information relating to the use of various psychoactive drugs and problems associated with such use. This will be followed by brief descriptions of the effects of some of the more well-known drugs commonly used today.
Physical dependence involves changes in normal bodily functions—the user will experience withdrawal from the drug upon cessation of use. In contrast, a person who has psychological dependence has an emotional, rather than physical, need for the drug and may use the drug to relieve psychological distress. Tolerance is linked to physiological dependence, and it occurs when a person requires more and more drug to achieve effects previously experienced at lower doses. Tolerance can cause the user to increase the amount of drug used to a dangerous level—even to the point of overdose and death.
Drug withdrawal includes a variety of negative symptoms experienced when drug use is discontinued. These symptoms usually are opposite of the effects of the drug. For example, withdrawal from sedative drugs often produces unpleasant arousal and agitation. In addition to withdrawal, many individuals who are diagnosed with substance use disorders will also develop tolerance to these substances. Psychological dependence, or drug craving, is a recent addition to the diagnostic criteria for substance use disorder in DSM-5. This is an important factor because we can develop tolerance and experience withdrawal from any number of drugs that we do not abuse. In other words, physical dependence in and of itself is of limited utility in determining whether or not someone has a substance use disorder.
DRUG CATEGORIES
The effects of all psychoactive drugs occur through their interactions with our endogenous neurotransmitter systems. Many of these drugs, and their relationships, are shown in Figure4.16. As you have learned, drugs can act as agonists or antagonists of a given neurotransmitter system. An agonist facilitates the activity of a neurotransmitter system, and antagonists impede neurotransmitter activity.
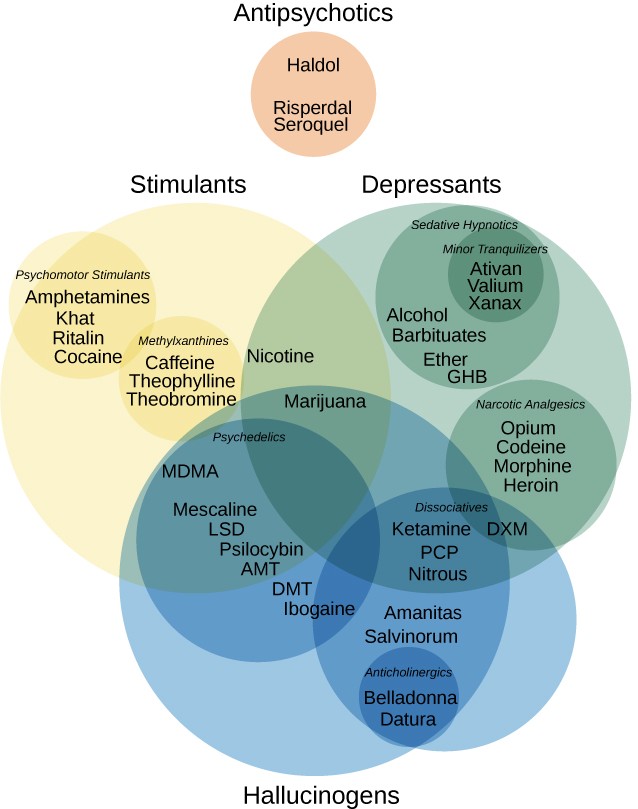
Figure 4.16 This figure illustrates various drug categories and overlap among them. (credit: modification of work by Derrick Snider)
Alcohol and Other Depressants
Ethanol, which we commonly refer to as alcohol, is in a class of psychoactive drugs known as depressants
(Figure 4.17). A depressant is a drug that tends to suppress central nervous system activity. Other depressants include barbiturates and benzodiazepines. These drugs share in common their ability to serve as agonists of the gamma-Aminobutyric acid (GABA) neurotransmitter system. Because GABA has a quieting effect on the brain, GABA agonists also have a quieting effect; these types of drugs are often prescribed to treat both anxiety and insomnia.
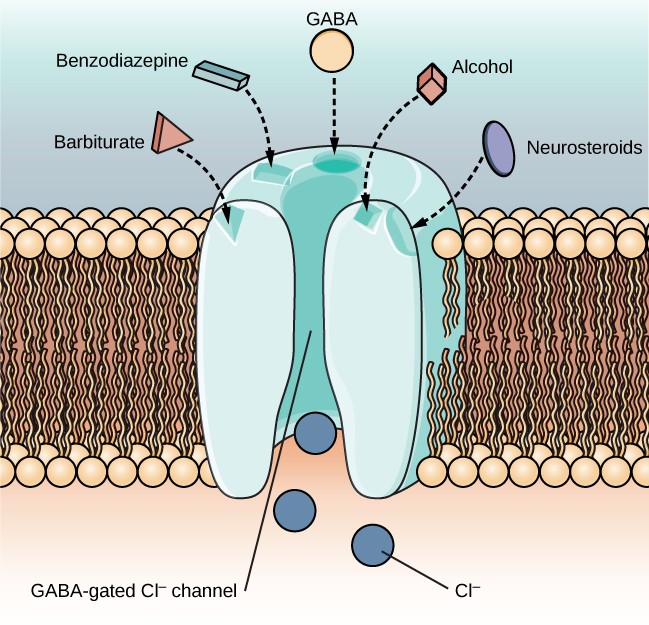
Figure 4.17 The GABA-gated chloride (Cl-) channel is embedded in the cell membrane of certain neurons. The channel has multiple receptor sites where alcohol, barbiturates, and benzodiazepines bind to exert their effects. The binding of these molecules opens the chloride channel, allowing negatively-charged chloride ions (Cl-) into the neuron’s cell body. Changing its charge in a negative direction pushes the neuron away from firing; thus, activating a GABA neuron has a quieting effect on the brain.
Acute alcohol administration results in a variety of changes to consciousness. At rather low doses, alcohol use is associated with feelings of euphoria. As the dose increases, people report feeling sedated. Generally, alcohol is associated with decreases in reaction time and visual acuity, lowered levels of alertness, and reduction in behavioral control. With excessive alcohol use, a person might experience a complete loss of consciousness and/or difficulty remembering events that occurred during a period of intoxication (McKim & Hancock, 2013). In addition, if a pregnant woman consumes alcohol, her infant may be born with a cluster of birth defects and symptoms collectively called fetal alcohol spectrum disorder (FASD) or fetal alcohol syndrome (FAS).
Stimulants
Stimulants are drugs that tend to increase overall levels of neural activity. Many of these drugs act as agonists of the dopamine neurotransmitter system. Dopamine activity is often associated with reward and craving; therefore, drugs that affect dopamine neurotransmission often have abuse liability. Drugs in this category include cocaine, amphetamines (including methamphetamine), cathinones (i.e., bath salts), MDMA (ecstasy), nicotine, and caffeine.
Cocaine can be taken in multiple ways. While many users snort cocaine, intravenous injection and ingestion are also common. The freebase version of cocaine, known as crack, is a potent, smokable version of the drug. Like many other stimulants, cocaine agonizes the dopamine neurotransmitter system by blocking the reuptake of dopamine in the neuronal synapse.
In recent years, methamphetamine (meth) use has become increasingly widespread. Methamphetamine is a type of amphetamine that can be made from ingredients that are readily available (e.g., medications containing pseudoephedrine, a compound found in many over-the-counter cold and flu remedies). Despite recent changes in laws designed to make obtaining pseudoephedrine more difficult, methamphetamine continues to be an easily accessible and relatively inexpensive drug option (Shukla, Crump, & Chrisco, 2012). Users can experience physical symptoms that include nausea, elevated blood pressure, and increased heart rate. In addition, these drugs can cause feelings of anxiety, hallucinations, and paranoia (Fiorentini et al., 2011).
Caffeine is another stimulant drug. While it is probably the most commonly used drug in the world, the potency of this particular drug pales in comparison to the other stimulant drugs described in this section. Generally, people use caffeine to maintain increased levels of alertness and arousal. Caffeine is found in many common medicines (such as weight loss drugs), beverages, foods, and even cosmetics (Herman & Herman, 2013).
Nicotine is highly addictive, and the use of tobacco products is associated with increased risks of heart disease, stroke, and a variety of cancers. Nicotine exerts its effects through its interaction with acetylcholine receptors. Acetylcholine functions as a neurotransmitter in motor neurons. In the central nervous system, it plays a role in arousal and reward mechanisms. Nicotine is most commonly used in the form of tobacco products like cigarettes or chewing tobacco; therefore, there is a tremendous interest in developing effective smoking cessation techniques. In general, smoking cessation programs may be effective in the short term, but it is unclear whether these effects persist (Cropley, Theadom, Pravettoni, & Webb, 2008; Levitt, Shaw, Wong, & Kaczorowski, 2007; Smedslund, Fisher, Boles, & Lichtenstein, 2004).
Opioids
An opioid is one of a category of drugs that includes heroin, morphine, methadone, and codeine. Opioids have analgesic properties; that is, they decrease pain. Humans have an endogenous opioid neurotransmitter system—the body makes small quantities of opioid compounds that bind to opioid receptors reducing pain and producing euphoria. Thus, opioid drugs, which mimic this endogenous painkilling mechanism, have an extremely high potential for abuse. Natural opioids, called opiates, are derivatives of opium, which is a naturally occurring compound found in the poppy plant. There are now several synthetic versions of opiate drugs (correctly called opioids) that have very potent painkilling effects, and they are often abused.
Historically, heroin has been a major opioid drug of abuse (Figure4.20). Heroin can be snorted, smoked, or injected intravenously. Like the stimulants described earlier, the use of heroin is associated with an initial feeling of euphoria followed by periods of agitation. Because heroin is often administered via intravenous injection, users often bear needle track marks on their arms and, like all abusers of intravenous drugs, have an increased risk for contraction of both tuberculosis and HIV.
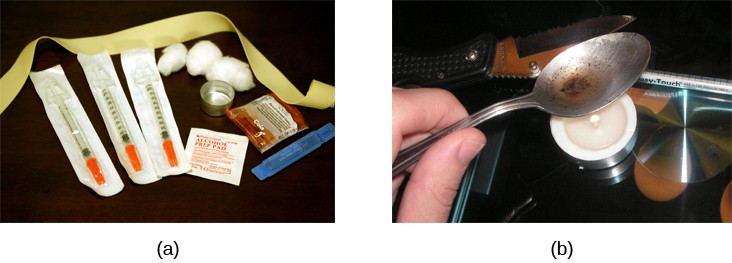
Figure 4.20 (a) Common paraphernalia for heroin preparation and use are shown here in a needle exchange kit. (b) Heroin is cooked on a spoon over a candle. (credit a: modification of work by Todd Huffman)
Aside from their utility as analgesic drugs, opioid-like compounds are often found in cough suppressants, anti-nausea, and anti-diarrhea medications. Given that withdrawal from a drug often involves an experience opposite to the effect of the drug, it should be no surprise that opioid withdrawal resembles a severe case of the flu.
Codeine is an opioid with relatively low potency. It is often prescribed for minor pain, and it is available over-the-counter in some other countries. Like all opioids, codeine does have abuse potential. In fact, abuse of prescription opioid medications is becoming a major concern worldwide (Aquina, Marques-Baptista, Bridgeman, & Merlin, 2009; Casati, Sedefov, & Pfeiffer-Gerschel, 2012).
Hallucinogens
A hallucinogen is one of a class of drugs that results in profound alterations in sensory and perceptual experiences (Figure 4.21). In some cases, users experience vivid visual hallucinations. It is also common for these types of drugs to cause hallucinations of body sensations (e.g., feeling as if you are a giant) and a skewed perception of the passage of time.

Figure 4.21 Psychedelic images like this are often associated with hallucinogenic compounds. (credit: modification of work by “new 1lluminati”/Flickr)
Other States of Consciousness
Learning Objectives
By the end of this section, you will be able to:
- Define hypnosis and meditation
- Understand the similarities and differences of hypnosis and meditation
Our states of consciousness change as we move from wakefulness to sleep. We also alter our consciousness through the use of various psychoactive drugs. This final section will consider hypnotic and meditative states as additional examples of altered states of consciousness experienced by some individuals.
HYPNOSIS
Hypnosis is a state of extreme self-focus and attention in which minimal attention is given to external stimuli. In the therapeutic setting, a clinician may use relaxation and suggestion in an attempt to alter the thoughts and perceptions of a patient. Hypnosis has also been used to draw out information believed to be buried deeply in someone’s memory. For individuals who are especially open to the power of suggestion, hypnosis can prove to be a very effective technique, and brain imaging studies have demonstrated that hypnotic states are associated with global changes in brain functioning (Del Casale et al., 2012; Guldenmund, Vanhaudenhuyse, Boly, Laureys, & Soddu, 2012).
Historically, hypnosis has been viewed with some suspicion because of its portrayal in popular media and entertainment (Figure 4.23). Therefore, it is important to make a distinction between hypnosis as an empirically based therapeutic approach versus as a form of entertainment. Contrary to popular belief, individuals undergoing hypnosis usually have clear memories of the hypnotic experience and are in control of their own behaviors. While hypnosis may be useful in enhancing memory or a skill, such enhancements are very modest in nature (Raz, 2011).
Figure 4.23 Popular portrayals of hypnosis have led to some widely-held misconceptions.
How exactly does a hypnotist bring a participant to a state of hypnosis? While there are variations, there are four parts that appear consistent in bringing people into the state of suggestibility associated with hypnosis (National Research Council, 1994). These components include:
- The participant is guided to focus on one thing, such as the hypnotist’s words or a ticking watch.
- The participant is made comfortable and is directed to be relaxed and sleepy.
- The participant is told to be open to the process of hypnosis, trust the hypnotist and let go.
- The participant is encouraged to use his or her imagination.
These steps are conducive to being open to the heightened suggestibility of hypnosis.
People vary in terms of their ability to be hypnotized, but a review of available research suggests that most people are at least moderately hypnotizable (Kihlstrom, 2013). Hypnosis in conjunction with other techniques is used for a variety of therapeutic purposes and has shown to be at least somewhat effective for pain management, treatment of depression and anxiety, smoking cessation, and weight loss (Alladin, 2012; Elkins, Johnson, & Fisher, 2012; Golden, 2012; Montgomery, Schnur, & Kravits, 2012).
MEDITATION
Meditation is the act of focusing on a single target (such as the breath or a repeated sound) to increase awareness of the moment. While hypnosis is generally achieved through the interaction of a therapist and the person being treated, an individual can perform meditation alone. Often, however, people wishing to learn to meditate receive some training in techniques to achieve a meditative state. A meditative state, as shown by EEG recordings of newly-practicing meditators, is not an altered state of consciousness per se; however, patterns of brain waves exhibited by expert meditators may represent a unique state of consciousness (Fell, Axmacher, & Haupt, 2010).
Although there are a number of different techniques in use, the central feature of all meditation is clearing the mind in order to achieve a state of relaxed awareness and focus (Chen et al., 2013; Lang et al., 2012). Mindfulness meditation has recently become popular. In the variation of meditation, the meditator’s attention is focused on some internal process or an external object (Zeidan, Grant, Brown, McHaffie, & Coghill, 2012).
Meditative techniques have their roots in religious practices (Figure 4.24), but their use has grown in popularity among practitioners of alternative medicine. Research indicates that meditation may help reduce blood pressure, and the American Heart Association suggests that meditation might be used in conjunction with more traditional treatments as a way to manage hypertension, although there is not sufficient data for a recommendation to be made (Brook et al., 2013).

Figure 4.24 (a) This is a statue of a meditating Buddha, representing one of the many religious traditions of which meditation plays a part. (b) People practicing meditation may experience an alternate state of consciousness. (credit a: modification of work by Jim Epler; credit b: modification of work by Caleb Roenigk)
Summary
What Is Consciousness?
States of consciousness vary over the course of the day and throughout our lives. Important factors in these changes are the biological rhythms, and, more specifically, the circadian rhythms generated by the suprachiasmatic nucleus (SCN). Typically, our biological clocks are aligned with our external environment, and light tends to be an important cue in setting this clock. When people travel across multiple time zones or work rotating shifts, they can experience disruptions of their circadian cycles that can lead to insomnia, sleepiness, and decreased alertness. Bright light therapy has shown to be promising in dealing with circadian disruptions. If people go extended periods of time without sleep, they will accrue a sleep debt and potentially experience a number of adverse psychological and physiological consequences.
Sleep and Why We Sleep
We devote a very large portion of time to sleep, and our brains have complex systems that control various aspects of sleep. Several hormones important for physical growth and maturation are secreted during sleep. While the reason we sleep remains something of a mystery, there is some evidence to suggest that sleep is very important to learning and memory.
Sleep Problems and Disorders
Many individuals suffer from some type of sleep disorder or disturbance at some point in their lives. Insomnia is a common experience in which people have difficulty falling or staying asleep. Parasomnias involve unwanted motor behavior or experiences throughout the sleep cycle and include RBD, sleepwalking, restless leg syndrome, and night terrors. Sleep apnea occurs when individuals stop breathing during their sleep, and in the case of sudden infant death syndrome, infants will stop breathing during sleep and die. Narcolepsy involves an irresistible urge to fall asleep during waking hours and is often associated with cataplexy and hallucination.
Substance Use and Abuse
Substance use disorder is defined in DSM-5 as a compulsive pattern of drug use despite negative consequences. Both physical and psychological dependence are important parts of this disorder. Alcohol, barbiturates, and benzodiazepines are central nervous system depressants that affect GABA neurotransmission. Cocaine, amphetamine, cathinones, and MDMA are all central nervous stimulants that agonize dopamine neurotransmission, while nicotine and caffeine affect acetylcholine and adenosine, respectively. Opiate drugs serve as powerful analgesics through their effects on the endogenous opioid neurotransmitter system, and hallucinogenic drugs cause pronounced changes in sensory and perceptual experiences. The hallucinogens are variable with regards to the specific neurotransmitter systems they affect.
Other States of Consciousness
Hypnosis is a focus on the self that involves suggested changes of behavior and experience. Meditation involves relaxed, yet focused, awareness. Both hypnotic and meditative states may involve altered states of consciousness that have potential application for the treatment of a variety of physical and psychological disorders.