
Aftereffects
Nazi Eugenics, Euthanasia, and Medical Ethics Today
Michael S. Bryant
Contents
- Pre-Nazi Period
- Eugenics in Germany
- Hitler and Eugenic Thought in the 1920s
- Nazi Eugenics: 1933-1939
- Nazi Eugenics in Action: the “Euthanasia” Program, 1939-41
- The T4 Killing Centers
- “Wild” Euthanasia, September 1941-April 1945
- Eugenics in Nazi-occupied Eastern Europe
- Medical Ethics and Nazi Eugenics
- Conclusion
- References
When I teach the Holocaust and post-war Nazi trials to undergraduates and law students, they are often most horrified by the medical experiments carried out in the concentration camps during the war. Their revulsion was shared by the chief American prosecutor of the Doctors Trial at Nuremberg, Telford Taylor, whose opening statement placed Nazi medical crimes in a category all their own:
The defendants…are charged with murder, but this is no mere murder trial. …To kill, to maim, and to torture is criminal under all modern systems of law. These defendants did not kill in hot blood, nor for personal enrichment. …They are not ignorant men. Most of them are trained physicians and some…are distinguished scientists. Yet [they]…are responsible for wholesale murder and unspeakably cruel tortures (Taylor 1946).
The “wholesale murder and unspeakably cruel tortures” that Taylor refers to did not occur in a vacuum; they were powered by ideas that, while corrupted and twisted to fit Nazi ideology, came down to Hitler and his followers from the 19th and early 20th centuries. Among these ideas, and most crucial for our discussion here of Nazi medical crimes, is “eugenics.” One does not have to be a Nazi to support eugenics. Indeed, some of the brightest and most compassionate minds have been sympathetic to it. Nonetheless, Nazism reveals the destructive potentiality of eugenics when a racist tyranny is inspired by its ideals. While allied armies destroyed Nazism in 1945, Nazi-like interpretations of eugenics persist until our own day. Nazi racial sciences, including eugenics, represent the lethal underbelly of modern science and its sometimes-heedless interference with the sources of life on our planet.
Pre-Nazi Period
We might begin our investigation into Nazi eugenics by delving into the roots of the phenomenon, which lie in the mid-19th century. In 1859 the British naturalist Charles Darwin (1809-1882) published one of the most important books in human history, On the Origin of Species by Means of Natural Selection, or the Preservation of Favoured Races in the Struggle for Life. In this work, Darwin set forth his theory of evolution through natural selection. He argued that animal and plant species able to adapt most efficiently to their environment over time were selected for survival while those that failed to do so died out. Popular spin-offs of his evolutionary theory like “survival of the fittest” and the “struggle for existence” spread throughout the Western world in the years following publication of his book. Herbert Spencer, the inventor of the phrase “survival of the fittest,” was one such popularizer of Darwin’s
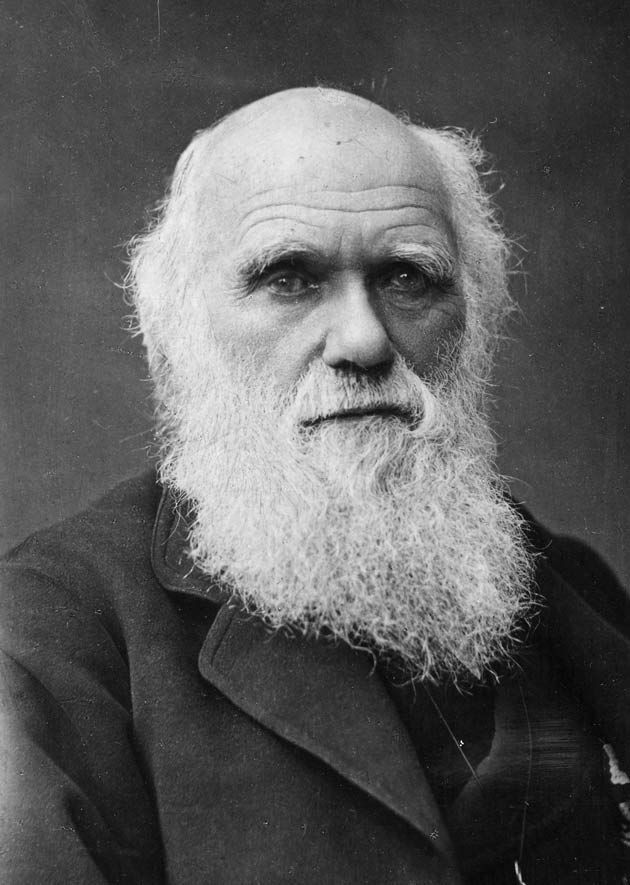
Source: Wikipedia, 2022
theory. Spencer believed he had found in Darwin scientific evidence that the state must not interfere with the “natural” growth of society by aiding the poor. To do so would violate the order of nature, in which the unfit were put to the wall and the fittest thrived. In nature, Spencer wrote, organisms that “are sufficiently complete to live…do live, and it is well they should live. If they are not sufficiently complete to live, they die, and it is best they should die.” If nature evolved toward higher and more complete life forms through natural selection, then the same logic should govern human society. On this basis, Spencer rejected state intervention to improve the lives of the weak and infirm, rejecting poor laws, public education, sanitary regulation, public housing initiatives, and consumer protection. (Spencer, 1864, pp. 414-15)
Social Darwinist notions of natural selection, progress, and elimination of the unfit fed the mounting fears of middle-class Westerners in the latter half of the 19th century that the West was declining. In the midst of these fears of societal decay Charles Darwin’s cousin, Francis Galton, invented the science of eugenics. Like Spencer, Galton extrapolated from the animal kingdom to human society, asking, “Could not the race of men be similarly improved? Could not the undesirables be got rid of and the desirables multiplied?” Galton coined the word “eugenics” to denote his program of selective breeding in his Inquiries into Human Faculty and Development (1883).
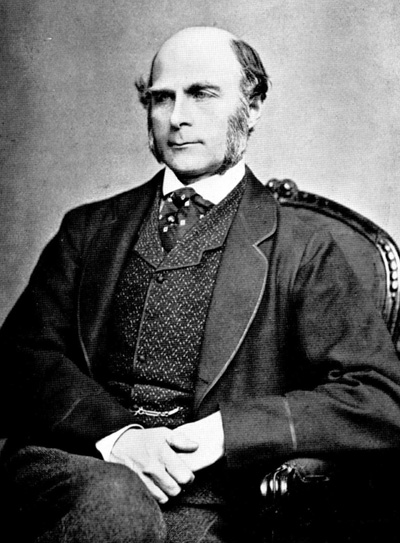
Foreshadowing later population policies under the Nazis, Galton held it would be “quite practicable to produce a highly gifted race of men by judicious marriages during several consecutive generations.” He proposed that the state promote weddings among the most gifted young people. Children of the marriages would receive government subsidies to cultivate their “natural ability.” This was the positive side of Galton’s ledger. On the negative side, he suggested that the “unfit” be prevented from reproducing (quoted. in Kevles, 1995, p. 4).
Victorian intellectuals like Spencer and Galton invoked Darwin’s conception of evolution through natural selection to explain individual and group inferiority among humans. The father of criminal anthropology, the Italian psychiatrist Cesare Lombroso, employed Social Darwinist ideas to argue that criminals were arrested at a primitive stage of human evolution. Criminals were, in fact, degenerates who reproduced ape-like characteristics. Lombroso was among the first researchers to establish a fateful link between career criminals and the mentally ill (Gould, 1996, p. 153). By measuring a person’s anatomy, Lombroso asserted we could tell who was an evolutionary throwback, prone to deviant acts. The inward tendency toward crime was visible on the physical bodies of the criminal— in the “high cheek bones,” “prominent” arches, “handle-shaped ears,” etc.— all of which constituted a visible index of criminality, savagery, and apishness. For Lombroso these physical traits were the signs of degeneration. It was in the very nature of such persons to be criminal (Lombroso, 1887, p. 667).
The work of Spencer, Galton, and other 19th century eugenicists affirmed a biological basis for social inequality; the work of Lombroso and his interpreters asserted a biological basis for social deviancy. Lombroso insisted that since “born criminals” were incorrigible it made little sense to punish them. Rather, society should “eliminate them completely, even by death.” The particular targets of Lombroso’s eliminationist thinking were not only individuals but also entire groups as well, whom he believed had congenital tendencies toward crime. Two such groups were the mentally handicapped and Gypsies. Regarding the mentally handicapped, Lombroso found that “almost every ‘born criminal’ suffers from epilepsy to some degree,” making epilepsy a “mark of criminality.” The Gypsies, on the other hand, were “vain, like all delinquents, but they have no fear or shame. … They have the improvidence of the savage and that of the criminal as well” (Friedlander, 1994, 3).
Much later, the Nazis will murder the mentally ill, alleged hereditary criminals they called “asocials,” and the Roma (“Gypsies”). Did Lombroso influence these subsequent programs of mass killing? We cannot say for certain, yet Lombroso’s ideas were circulated throughout Germany in the late 19th century. His book L’uomo delinquato or Criminal Man (Italian) was first published in 1876. It was translated into German along with his other works in the 1890s. Inspired by Lombroso’s theories, German researchers probed the brain tissues of murderers for abnormalities. Apostles of Lombroso’s ideas in Germany founded a movement for criminal biology in the 1890s dedicated to “scientific” theories of crime prevention. The weekly journal Die Zukunft “The Future” disseminated his teachings to the German public (Weindling, 1989, pp. 82-83). Presumably, the teachers of future Nazi doctors were exposed to Lombroso’s ideas during their professional training at the turn of the century.
By 1900, the eugenic goal of ‘eliminating valueless life’ could be attained in one of three ways: (1) by abandoning the poor and infirm to the forces of “nature,” resulting in their destruction through natural selection (Spencer); (2) by preventing “inferiors” from breeding (Galton); or (3) killing them (Lombroso). Yet, despite the proliferation of these ideas, organized killing of “valueless” life did not occur until the late 1930s. Industrialization and modernity created the vine on which eugenic ideologies grew; a catastrophic world war was required for the eugenic fruit to ripen into full-fledged programs of mass-murder.
Eugenics in Germany
Scholars of Nazi eugenics identify the First World War (1914-1918) as a major turning point in the history of the Nazi assault on “unworthy life” (See, e.g., Klee, 1986, p. 18; Friedlander, 1994, p. 12; Burleigh, 1991, p. 34; Proctor, 1988, p. 178). Before 1920, proposals to use state power to eliminate unwanted people from a society believed to be collapsing were on the fringes of public discourse. The radicalizing effects of the Great War, however, pushed these outliers from the fringe toward the center. From 1920 until Hitler came to power in 1933, increasing numbers of Germans were won to the cause of violent solutions to the problem of mental disability.
Already in the 1890s, voices from the fringe in Germany were calling for the direct killing of incurably ill and mentally handicapped patients. In 1895, Adolf Jost argued for two death-dealing rights in his book The Right to Death: the right of terminally ill persons to end their sufferings through voluntary euthanasia and the right of the state to end the lives of the incurable and mentally defective. The state, Jost contended, should be permitted to destroy individuals who had become a burden on society and their relatives, even when they were unable to express their wishes for euthanasia. Jost grounded the right of the state to kill patients in its right to sacrifice young men in times of war for the welfare of the state. Jost’s book illustrates how German theorists of biological inferiority confused separate issues. The dignified right of a terminally ill person to choose euthanasia as an alternative to continued suffering and painful medical intervention was conflated with the state’s power to kill nonterminal patients because they are a financial burden. This style of thought—the tendency to confuse distinct questions and demand a common answer for each—would be typical of the planners and policymakers who implemented the “euthanasia” program during World War II (Burleigh, 1994, p. 12; Lifton, 1986, p. 46).
Jost and other advocates of violence against the disabled were largely ignored until after World War I. The catastrophic impact of the Great War on the generation of Germans who experienced it cannot be overstated. The militarism, mass-death, economic distress, defeat, and— perhaps most importantly—code of violence produced by the Great War would all leave their mark on the future perpetrators of Nazi crimes. The influence would prove far-reaching, extending not only to the leadership corps of the Nazi Party but also to physicians, mental institution directors, nurses, and public health officials.
By 1920, the injurious effects of World War I had altered the moral landscape within German medicine. The chairman of the German Psychiatric Association, Karl Bonhoeffer, discussed this change in his inaugural address before the Association in 1920:
It could almost seem as if we have witnessed a change in the concept of humanity. I simply mean that we were forced by the terrible exigencies of war to ascribe a different value to the life of the individual than was the case before, and that in the years of starvation during the war we had to get used to watching our patients die of malnutrition in vast numbers, almost approving of this, in the knowledge that perhaps the healthy could be kept alive through these sacrifices. But in emphasizing the right of the healthy to stay alive, which is an inevitable result of periods of necessity, there is also a danger of going too far: a danger that the self-sacrificing subordination of the strong to the needs of the helpless and ill, which lies at the heart of any true concern for the sick, will give ground to the demand of the healthy to live (Bonhoeffer, 1920, qtd. in Burleigh, 1994, pp. 111-12).

Changing attitudes toward the value of individual life cleared a path for the single most influential document in Nazi attitudes toward the disabled—a pamphlet entitled The Permission to Destroy Life Unworthy of Life, published in 1920. An eminent retired jurist from the University of Leipzig, Karl Binding (1841-1920), and a professor of psychiatry at the University of Freiburg, Alfred Hoche (1856-1944), were the co-authors of the tract. It was divided into two sections, one written by Binding, the other by Hoche. Binding started his section with a defense of the individual’s right over his or her body—an overarching right that entailed the right to suicide. Although he conceded the interest of society in preserving valuable members, the right of a terminally ill patient experiencing intense pain to have a physician end his or her life by artificial means overrode the social interest. While he emphasized that euthanasia in such a case had to be consensual, the principle of autonomy was at war with his conception of “valueless” life. He asked: “Is there human life which has so far forfeited the character of something entitled to enjoy the protection of the law that its prolongation represents a perpetual loss of value, both for its bearer and for society as a whole?” (qtd. in Burleigh, 1994, p. 15-17) The question is of course rhetorical. By posing it, Binding has confused an issue involving a competent terminally ill patient with whether individuals may be destroyed whose lives are deemed valueless. He treats the two issues as constituting a common problem calling for a common solution.
Binding identified the three groups who qualified for his proposed euthanasia measures: (1) terminally ill patients (including the mortally wounded) who expressed their wish for a premature death; (2) “incurable idiots,” no matter whether their idiocy was congenital or acquired; and (3) people who had suffered grievous physical war injuries that rendered them unconscious, but who would desire a foreshortening of their lives if they were able to express their wishes. These three groups represented a class of individuals Binding called lebensunwertes Leben “life unworthy of life”, an ambiguous phrase that apparently covered persons whose lives had been made unbearable because of physical pain and persons whom society regarded as so defective by virtue of their mental impairment that their lives had no value. Holocaust historian Henry Friedlander accuses Binding and his supporters of conscious prevarication here: they deliberately cloud the debate “by pointing to the suicide rights of terminal cancer patients facing a certain and painful death when in reality they wanted to ‘destroy’ the ‘unworthy life’ of healthy but ‘degenerate’ individuals” (Friedlander, 1994, p. 15). If Friedlander is correct, then Binding and Hoche’s tract is little more than advocacy of killing people whom the state considered “unworthy of life” under the guise of a humanitarian concern for their suffering.
Binding ended his contribution to the tract with an outline of the procedures to govern the proposed killing program. The patient, the doctor, or the patient’s relatives could initiate a request for euthanasia, but only the state could authorize it. Binding provided for a panel of “experts” consisting of a jurist and two doctors responsible for evaluating each application. Their decision, Binding stipulated, had to rest on the most current scientific knowledge, the mode of killing had to be “absolutely painless,” and the person administering the killing had to be an expert. Errors would doubtlessly occur, but Binding brushed them aside (Binding/Hoche, 1920, pp. 39-40).
Binding and Hoche’s work provoked debate among lawyers, doctors, and theologians in Weimar Germany. Tübingen psychiatrist Robert Gaupp seized on Binding/Hoche’s economic justifications to argue that the Christian notion of the sanctity of life had to be revised in view of the economic distress caused by the Versailles Treaty. A 1920 address to the Society for Forensic Medicine by the Berlin judge Karl Klee reflected the Binding/Hoche thesis in its proposal to ground capital punishment in its tendency to purify the nation of “parasitic existences” (qtd. in Burleigh, 1994, p. 20). Notwithstanding these and other advocates of Binding/Hoche, the idea of destroying “life unworthy of life” was fiercely contested during the Weimar era, nor did it find an official foothold in Germany until the late 1930s. Numerous opponents refuted their arguments, pointing to the dubious business of assigning degrees of value to human life and to the inflationary potential inherent in such an arrogation of power by the state (Burleigh, 1994, pp. 21-22).
The German medical profession, too, remained opposed to the Binding/Hoche thesis during the Weimar Republic. The “change in the concept of humanity” that Karl Bonhoeffer had noticed in the aftermath of World War One, however, gradually crept over the German medical community in the 1920s. Perhaps the most significant contribution to this “change in the concept of humanity” was a shift of the doctor’s duty from the individual patient to the “body of the people” (Volkskörper). Late 19th-century eugenics had, of course, always subordinated the individual to the wellbeing of the collective, conceived as state, society, nation, or, in Germany, as das Volk or “the people”.
The prewar German eugenics movement, unlike its decentralized counterparts in the United States and Great Britain, was concentrated in a single group, the German Society for Race Hygiene. Its journal, the Archive for Racial and Social Biology, was the leading forum for eugenic ideas in Germany. The German Society shared with American and British eugenicists a belief in congenital “superiority” and “inferiority,” making it the Society’s task to preserve Germany’s “genetic heritage” from biological degeneracy. Prior to the Great War, German eugenicists had de-emphasized the negative implications of their beliefs (i.e., primarily sterilization of the unfit), realizing that little support existed for it in the population, and focused instead on promoting the health of the nation by raising the birth rate of “superior” individuals (Friedlander, 1994, pp. 9-10). Germany’s military collapse, however, radicalized German eugenics. Among physicians, emphasis shifted from the individual as the object of medical treatment to the “body of the people.” Since German eugenicists tended to be physicians and academic psychiatrists working in state hospitals and university clinics, this meant that caregivers directly responsible for the mentally disabled were abandoning the Hippocratic ethic of devotion to their patients’ wellbeing.
This process of radicalization demonstrates that the ideology of biological value was not confined to Nazism but circulated in Germany and throughout Western industrial nations well before Hitler came to power in 1933. Without Hitler’s seizure of power, however, the dream of eliminating the “inferiors” would likely have never been realized. For Nazism was the most powerful host in which lurked the virus of eugenic mass murder.
Hitler and Eugenic Thought in the 1920s
Adolf Hitler was exposed to eugenic ideas at least as early as 1923, when during his time in prison he read what would become a classic text of scientific racism, the Outline of Human Genetics and Racial Hygiene. Two of the authors of the book— Eugen Fischer and Fritz Lenz—were deeply involved in the Nordic wing of the Race Hygiene Society in Germany. (The third author. Erwin Baur, was an eminent botanist and chief of the Kaiser Wilhelm Institute for Plant Cultivation and Genetic Research.) This wing of German eugenics regarded the Nordic (or Germanic) peoples as superior to all other racial groups. In the 1920s German Nordic eugenicists referred to their “scientific” hierarchies of racial value as either “race hygiene” or “eugenics.” After 1933 the Nordic faction would dominate German eugenics, adopting for the first time an aggressive anti-Semitism and making “Race Hygiene” the sole designation for German eugenics (Friedlander, 1994, pp. 11-13; Weindling, 1989, p. 397)
Hitler recorded the influences of this text in his autobiography Mein Kampf, “My Struggle,” (1925/27), in which he argued that all of history was a feral struggle for existence. Displaying the degree to which trench warfare had brutalized his thought, he conceived of the universe as driven forward to higher levels of development through ferocious conflict. We read:
Nature…puts living creatures on this globe and watches the free play of forces. She then confers the master’s right on her favorite child, the strongest in courage and industry…. Only the born weakling can view this as cruel, but he after all is only a weak and limited man: for if this law did not prevail, any conceivable higher development of organic living beings would be unthinkable…. In the end, only the urge for self-preservation can conquer. Beneath it so-called humanity, the expression of a mixture of stupidity, cowardice, and know-it-all conceit, will melt like snow in the March sun. Mankind has grown great in eternal struggle, and only in eternal peace does it perish. (Hitler, Mein Kampf, qtd. In J. Fest, 1974, p. 215)
In his Tischgespräche or “Table Talks, Hitler inferred from this violent “Law of Nature” a justification for “all imaginable means” in the struggle between national groups, including “persuasion, cunning, cleverness, persistence, kindness, wiliness, and brutality” (Hitler, qtd. in Fest, 1974, p. 219). For Hitler in both Mein Kampf and his speeches, the ends justified the means since the future of humanity hung in the balance. By disregarding nature’s law whereby the strong destroyed the weak and mated only with their own kind (the “titmouse seeks the titmouse, the finch the finch, the stork the stork, the field mouse the field mouse”), higher civilizations throughout history had ensured their own decline and fall. Only by restoring the law of nature to German society could the Aryans preserve their racial stock, and only in this way could true humanity, identified with the cause of the Aryan, be advanced. The alternative was decadence, decay, and death (Hitler, qtd. in Fest, 1974, 220).
While Hitler singled out the Jews as the Aryans’ racial archenemy, there is an implicit hostility in Mein Kampf toward all groups perceived by the Nazis to be strange or alien. Hitler did not write about killing biological “inferiors” like the mentally disabled in Mein Kampf, but the premise that Germany could only avoid cultural extinction by abandoning the weak to the “law of nature” threatened at best indifference, at worst violent intervention by the state once the Nazis came to power. By the late 1920s, the implications of Hitler’s worldview in Mein Kampf had crystallized into specific utterances about killing the mentally disabled. In 1928 Hitler commended the Spartans for putting to death deformed children, claiming that their military strength derived from the practice of weeding out “defectives” (Hitler, qtd. in Weinberg, 1961, pp. 56-7). The late-1920s may have been the time when the notions of war readiness and elimination of the “unfit” converged in Hitler’s mind. During a party rally at Nuremberg in 1929, Hitler railed against the social welfare state for breeding “inferiors” and destroying the strong. This situation could be corrected, he suggested, by wiping out a million “burdensome lives” (Weindling, 1989, p. 545).
Nazi Eugenics: 1933-1939
The Nazi assault on the mentally disabled began shortly after Hitler became Chancellor in January 1933. It started with a governmentally mandated program of eugenic sterilization. During the Weimar years, the topic of eugenic sterilization was discussed among all political parties. The Social Democratic Party of Germany (SPD) supported voluntary sterilization as a way to curb poverty and alleviate the strain on social resources of surplus and hereditarily ill children. The Communists (KPD) similarly endorsed a program of consensual sterilization for health and social reasons. German right-wing parties like the Nazis and the German Nationalist People’s Party (DNVP) were firm adherents of eugenic sterilization. Despite this broad consensus on the value of sterilization, the Nazis were its foremost advocates. In 1931, Hitler identified sterilization as “the most humane act for mankind,” urging his listeners to overcome their misplaced pity and misgivings about it. His call to sterilize a substantial number of the German population was endorsed by eugenicists like Ernst Rüdin (the chief designer of the Nazi sterilization law passed in July 1933) and Fritz Lenz, the co-author of the Outline of Human Genetics and Racial Hygiene that had influenced Hitler during his Landsberg prison term in 1923. Years later, Rüdin would laud Hitler for being the only politician to introduce “the importance of eugenics…to all intelligent Germans…It was only through him that our more than thirty-year-old dream has become a reality and racial-hygiene principles have been translated into action.” Prominent Nazi party members like Alfred Rosenberg, Walter Gross, Walter Darré, and Dr. Leonardo Conti took up the cause in their public addresses (Weindling, 1989, p. 454).
Prior to 1933, involuntary eugenic sterilization remained an act of criminal assault under German law. With political power came the opportunity to change the status quo. On July 14, 1933, the Reich Ministry of the Interior presented to the cabinet a sterilization law, entitled “Law for the Prevention of Offspring with Hereditary Diseases.” Hitler backed the law but waited until the Catholic Concordat had been achieved on July 20, 1933, before publishing it on July 26,1933, to become effective on January 1, 1934. The law was modeled on an earlier Prussian proposal from 1932, with the critical difference that the Nazi variant did not require the consent of the affected person. In its final form, the law omitted reference to sterilizing or castrating “hereditary criminals” upon the recommendations of the Reich Justice Minister, who objected to a common law covering both the disabled and criminals (Weindling, 1989, pp. 545-25). In fact, the Nazis would deal with the problem of criminals through a separate law, as we will shortly see.
The law made it legally permissible to sterilize any person “if medical knowledge indicates that his offspring will suffer from severe hereditary physical or mental damage.” It then enumerated the categories of affliction recognized as grounds for sterilization: “(1) congenital feeblemindedness; (2) schizophrenia; (3) manic-depressive psychosis; (4) hereditary epilepsy; (5) Huntington’s chorea; (6) hereditary blindness; (7) hereditary deafness; (8) severe hereditary physical deformity; or (9) severe alcoholism on a discretionary basis.” It went on to establish a legal procedure for sterilization: the mentally handicapped patients themselves, public health service doctors, and directors of hospitals, nursing homes, and prisons were all competent to apply for sterilization under the new guidelines. Hereditary health courts would receive and evaluate all applications. Each court was attached to a local court of general jurisdiction and consisted of three members: a judge, a doctor from the public health service, and a physician specializing in genetics. An appellate system to handle cases on appeal was built into the regional appellate courts; a similar triad of one judge and two doctors constituted these courts of appeal, the decisions of which were final and non-appealable (Friedlander, 1994, 26).
As previously noted, the law contemplated both voluntary and involuntary sterilization. A positive finding by the courts permitted local health authorities throughout Germany to institute surgical procedures to sterilize the person, whether or not consent was given. With the passage of the law, nonconsensual sterilization ceased to be a criminal assault and battery; in fact, now physicians and public health officials could invoke the police power to enforce compliance. In the years following passage of the law, these local and state doctors and administrators had tens of thousands of German men and women involuntarily sterilized. In 1934, the majority (52.9 percent) were the “feeble-minded,” followed by those diagnosed with schizophrenia (25.4 percent) and epilepsy (14 percent). The criteria for a presumptive case of feeblemindedness were lying, argumentativeness, laziness and receptiveness to influence. The overarching issue, however, was the question of the person’s value to the Volk: if a case could be made for the person’s social usefulness, sterilization might be avoided; if not, then the decision was made to proceed (Weindling, 1989, p. 533; Friedlander, 1994, pp. 28-29; Bock, 1986, pp. 324-25). The inflationary potential for including ever greater numbers of people in this largest of the sterilization categories should be clear. It prefigures the expansive direction the “euthanasia” program would take in the 1940s as it first affected mentally ill children, then mentally ill adults, and later Jews, Gypsies, shell-shocked residents of bombed-out cities, and so-called “asocials.”
Subsequent amendments to the sterilization law enabled the state to eliminate “defectives” even where hereditarily “flawed” women had become pregnant before sterilization. In September 1934 Gerhard Wagner, the Reich Physician leader, informed German physicians that Hitler would relieve them from civil or criminal liability for abortions performed on women with hereditary defects. Immunity also extended to cases in which the mother was healthy, but the father suffered from a genetic abnormality. Wagner’s advisement was incorporated into the sterilization law as an amendment on June 26, 1935. The original law had empowered state authorities to restrict the mentally disabled by preventing them from having children; the amendment empowered them to eliminate “undesirables” in utero (Friedlander, 1994, p 30).
The wave of legislation between 1933 and 1936, of which the sterilization law was a part, identified categories of “unworthy life” that would become the targets of the Nazis during the war. The Law for the Prevention of Offspring with Hereditary Diseases, published in July of 1933, was followed by another four months later, the Law Against Dangerous Habitual Criminals and Regulation of Security and Reform, which was enacted on November 11, 1933. Section 42 of this law provided that “asocials” could be detained in mental institutions if they were deemed by the courts to have committed their crimes in a state of diminished responsibility. It also permitted the authorities to detain recidivists in public workhouses and detoxification centers and required castration for sexual offenders. Finally, the law forbade offenders from working in their professions (Aly, 1994, p. 59).

Additional legislation aimed at preventing the reproduction of disadvantaged groups followed two years later, when the regime enacted the Law for the Protection of German Blood and Honor (constituting, along with the Reich Citizenship law, the “Nuremberg Laws”). The law sought inter alia to eliminate Jews from the German folk community by illegalizing marriages Karl Brandt, Hitler’s escort physician and a principal organizer of the Nazi “euthanasia” program. Source: Wikipedia, 2022.
between Jews and Germans, as well as forbidding extramarital sexual relations between them. Further, it prohibited Jews from hiring German females as domestic help unless they were 45 years of age or older (apparently to prevent Jewish “lechers” from seducing and impregnating young German women). While the thrust of the Nuremberg Laws was directed against Jews, they were not the only group that fell within its purview. Although the text of the Blood Protection law only singled out Jews, article 6 was elastic enough to cover other groups: official commentators like Reich Minister of the Interior Wilhelm Frick interpreted article 6 ’s “other racially alien blood” to include “Negroes and Gypsies” (Friedlander, 1994, pp. 24-25; Gütt, Linden, and Massfeller, qtd. in Klee, 1986, p. 37).
Nazi Eugenics in Action: the “Euthanasia” Program, 1939-41
The Children’s Program, 1938-41
The decision to kill mentally ill patients was made sometime during the summer of 1939, probably in July. As early as 1938, however, the Nazi government had participated in the destruction of mentally handicapped children. In that year, a severely handicapped child from a family called “Knauer” was admitted to the Children’s Clinic at Leipzig University. (Subsequent research has revealed the true name of the family: Kretschmar.) The child’s father requested that the director, Werner Catel, euthanize the child, a request that Catel declined on legal grounds. The father then applied directly to Hitler through his private chancellery for permission to kill the child. Hitler was intrigued by the case, and sent his escort physician, Karl Brandt, to see the child to determine whether it was as severely handicapped as the family claimed in their petition. Brandt traveled to Leipzig, confirmed the doctors’ diagnosis, and authorized them to euthanize the child, which was done shortly thereafter. Hitler authorized Brandt and the Chief of the Führer’s Chancellery, Philip Bouhler, to take the same actions in all future cases of a similar nature. The Knauer case, as it was called, inaugurated the so-called “Children’s Operation,” a program designed to kill mentally and physically handicapped children (Friedlander, 1994, p. 39).
The Führer’s Chancellery would become the leading organizer and administrator of Nazi euthanasia (including the children’s operation), but it was not the only governmental office involved in the killing process. Department IV (“Public Health Service and Care of the Volk”) of the Reich Ministry of the Interior became the sole non-Party office to participate in the euthanasia program.
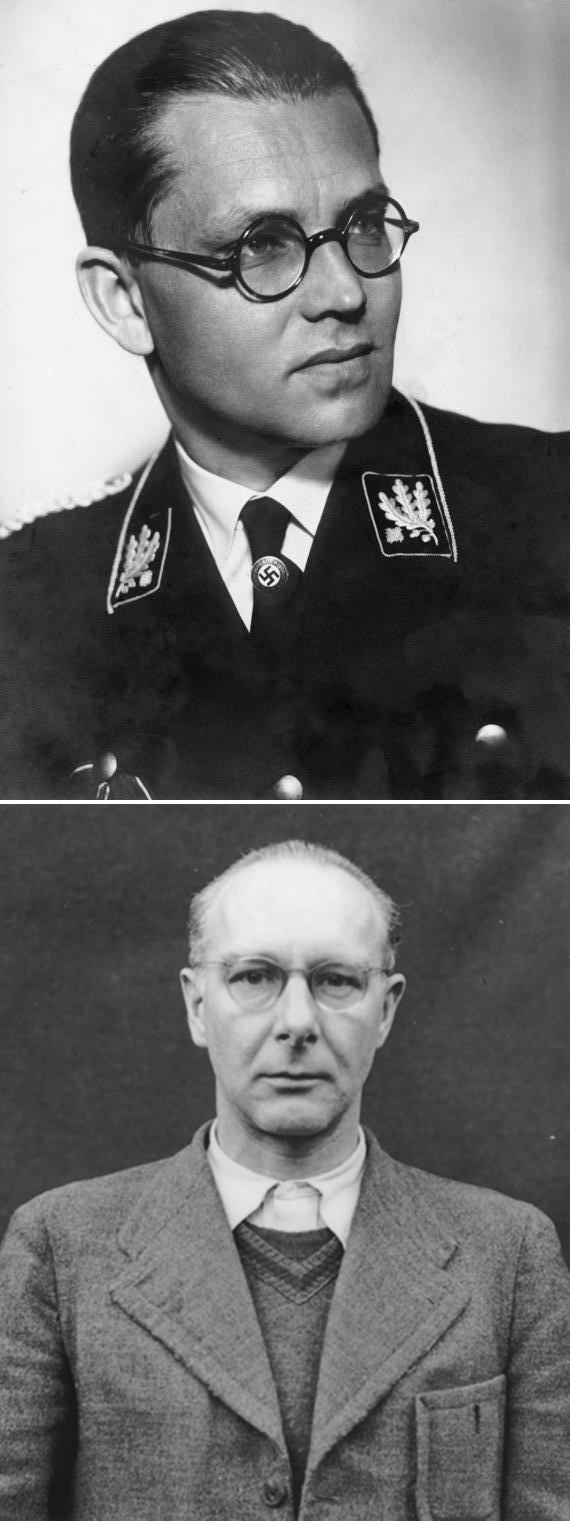
Department IV oversaw the local health administrations of the individual German states and supervised the state mental hospitals. From the earliest years of the Nazi regime, it was no stranger to state violence against the disabled: as part of its mandate to improve the public health, it had been an enforcer o f the government’s racial and eugenic laws. Prior to retiring in 1939, the chief of Department IV, Dr. Arthur Gütt, had been a steadfast advocate of Nazi race and eugenic theories, co-authoring two commentaries on the Nuremberg laws. Gütt’s successor was Dr. Leonardo Conti, erstwhile physician of the “martyred” Horst Wessel and founder of the Nazi Doctor’s Association in Berlin. Like Gütt, Conti was an adherent of the Nazi world view: asked about the Nazi law published in 1938 barring Jewish doctors from treating Aryans, Conti replied, “It is only the elimination of the Jewish element which provides for the German doctor the living space due to him.” One level below Gütt (and later Conti) in Department IV was Dr. Herbert Linden, who served as a section chief at the rank of ministerial councillor. As section chief Linden superintended state hospitals, nursing homes, and the regime’s marital and sterilization legislation. In addition, he had been a coauthor with Gütt on one of the latter’s commentaries on the Nuremberg and sterilization laws. Thus, the jurisdictional competence, along with the eugenic interests of Department IV’s directors, drew the Reich Ministry of the Interior into collaboration with the euthanasia program (Friedlander, 1994, 43).
Shortly after the Knauer case had been addressed in 1938, Viktor Brack, Hans Hefelmann, and Herbert Linden met to discuss the commission that Hitler had given Brandt and Bouhler. They developed a plan of action, then expanded the planning group to include pro-euthanasia doctors— Karl Brandt, Werner Catel, Hans Heinze, Hellmuth Unger, and Ernst Wentzler. The reasons for the inclusion of these five men are straightforward. Brandt had been involved in the Knauer case and< Bouhler for euthanasia; Catel had been director of the Leipzig clinic where the Knauer baby was born. Heinze was a psychiatrist and neurologist in charge of the Brandenburg-Görden state hospital, whom Linden had recommended for inclusion in the planning group. Unger, an opthamologist, had written a novel called Mission and Conscience that advocated euthanasia. (The novel was later adapted as a screenplay for the propaganda film “I Accuse,” intended to generate support among the German people for “mercy killing.”) Wentzler was a Berlin pediatrician recommended by the Reich Health Leader. Leonardo Conti (Klee, 2001, p. 68; Friedlander, 1994, p. 44).
| Physician | Institution | Pseudonym |
|---|---|---|
| Viktor Brack | Hitler’s Chancellery, Office IIb | Jennerwein |
| Werner Blankenburg | Deputy to Brack Office IIb | Brenner |
| Ernst Baumhard | Grafeneck and Hadamar | Dr. Jäger |
| Friedrich Berner | Hadamar | Dr. Barth |
| Kurt Borm | Sonnenstein and Bernburg | Dr. Storm |
| Heinrich Bunke | Brandenburg and Bernburg | Dr. Schneider |
| Klaus Endruweit | Sonnenstein | Dr. Bader |
| Hans-Bodo Gorgass | Hadamar | Dr. Kramer |
| Günther Hennecke | Grafeneck and Hadamar | Dr. Ott |
| Rudolf Lonauer | Hartheim | unknown |
| Georg Renno | Hartheim | unknown |
| Kurt Schmalenbach | Sonnenstein | Dr. Blume |
| Horst Schumann | Grafeneck and Sonnenstein | Dr. Keim |
| Aquilin Ulrich | Brandenburg | Dr. Schmitt |
| Ewald Worthmann | Sonnenstein | unknown |
From its earliest stages, the program was labeled a “secret Reich matter.” Subsequent initiates into the program, especially at the field level, were admonished that divulging the details of the euthanasia campaign to unauthorized persons would result in the severest punishment, possibly even the death penalty. The most striking feature of the Nazis’ deception was the elaborate structure of camouflage organizations they developed to hide the central role of Hitler’s personal chancellery in the killing. The members of the group planning the children’s euthanasia realized that an organization so closely connected to Hitler should not be the direct source of orders to kill handicapped children— at least not on the surface. Accordingly, they invented a camouflage body with a speciously scientific name: the Reich Committee for the Scientific Registration of Severe Hereditary Ailments. This organization, it must be stressed, was purely fictitious; from its origins, its sole purpose was to mask the involvement of the members of the Führer’s Chancellery in systematic murder. In fact, the nominal heads of the Reich Committee were two high-ranking Chancellery officials, Hans Hefelmann, chief of Office lIb of the Führer’s Chancellery, and his deputy, Richard von Hegener. To thicken the fog of secrecy, Hefelmann and von Hegener used the pseudonym “Dr. Klein” in all correspondence issued under the name of the Reich Committee relating to euthanasia. The practice of using false names was common among euthanasia officials and physicians during the war (Klee, 2001, p. 68; Friedlander, 1994, p. 44). (See Table 1)
In addition to creating the Reich Committee, the euthanasia planning group was faced with a logistical problem: how would the killing experts in the Führer’s Chancellery know precisely who qualified for destruction and where they were to be found? The problem was solved with the introduction of a registration system, based on which infant patients would be selected for killing. Registration forms would be sent to mental hospitals, nursing homes, and pediatric clinics throughout Germany, where the on-site medical staff would fill them out for each of their patients and return them to the “Reich Committee.” The forms arrived at a post office box in Berlin; from there, Hefelmann and von Hegener picked them up for distribution to a group of experts for review. Sometime in the summer of 1939, this planning phase came to an end. Meditating on the impending war against Poland, Hitler may have felt it was time to initiate the killing program he had mentioned to Gerhard Wagner in 1935. The first systematic killings of handicapped children would occur in October 1939—scarcely one month after the war had started (Klee, 2001, p. 68; Friedlander, 1994, p. 44).
The Reich Ministry of the Interior stiffened the enforcement arm of the euthanasia planners with a decree on August 18, 1939, the “Requirement to Report Deformed etc. Newborns.” The decree, like virtually everything connected with the killing program, was designated a “secret Reich matter,” a status that explained why it did not appear in the official ministry gazette. Its source was Department IV of the Interior Ministry. The decree enjoined all midwives and physicians to report to the competent local health office newborns and children under the age of three “suspected” of suffering from the following “congenital” illnesses:
- idiocy as well as mongolism (especially cases involving blindness and deafness),
- microcephaly,
- hydrocephaly of a severe and advanced degree,
- deformities of every kind, especially missing limbs, severely defective closure of the head and the vertebrae, etc.,
- paralysis, including Little’s Illness [i.e., spastic diplegia] (reproduced in Klee, 1986, p. 80; see also Friedlander, 1994, p. 45).
Attached to the decree was a reporting form to be filled out by the health care provider. The form required, among other things, the name, age, and sex of the child, a description of its illness, the impact of the illness on its ability to function in the hospital, its estimated life expectancy, and the prognosis for improvement. Once health care providers had completed and forwarded these reports to local health officials, they were sent to the Reich Committee postbox in Berlin for evaluation by the experts.
Once the forms arrived in Berlin, Hefelmann and von Hegener of the Führer’s Chancellery, Office II b, collected and sorted them. Although neither man had a medical background, they selected the forms deemed appropriate for review and passed them on to three experts in the Führers Chancellery: Werner Catel, Hans Heinze, and Ernst Wentzler. We have already encountered this trio in our discussion of the euthanasia planning group; each was a committed advocate of killing the mentally disabled. The Führer’s Chancellery attached its own form to every copy of the incoming reports. It bore the letterhead of the fictitious “Reich Committee” and contained little space for explanatory comments. A cryptic coding system determined the life or death of the child: a plus sign (+) meant that the child was to be killed, a minus sign (—) signified that the child’s life would be spared. Final decision about uncertain cases was deferred with the word “observation.” In the absence of carbon copies, the same form along with the original report were sent to each of the three experts for review and notation—meaning that each expert knew how the others had voted (Friedlander, 1994, pp. 45 ff.).
When the experts arrived at a positive finding, the “Reich Committee” (in reality, the officials of the Führer’s Chancellery) wrote to the local public health office with orders to prepare the selected child for transport to one of several “children’s wards” established in state mental institutions and clinics throughout Germany. The sole purpose of these children’s wards was to “euthanize” mentally and physically disabled children. The first was erected at Brandenburg-Görden near Berlin under the direction of the Hitler Chancellery expert Hans Heinze. Subsequently, children’s wards were erected in clinics in Leipzig, Niedermarsberg, Steinhof (Vienna), and Eglfing-Haar; during the war, others were established in Waldniel, Ansbach, Berlin, Eichberg, Hamburg, Kalmenhof, Kaufbeuren, Hadamar, Grossschweidnitz, Loben, Lüneburg, Meseritz-Obrawalde, Schleswig, Schwerin, Stadtroda, Stuttgart, Uchtspringe, and am Spiegelgrund (Vienna). There were approximately thirty such children’s wards, staffed with medical personnel recruited for killing by the Führer s Chancellery. Hefelmann and von Hegener of the Führer’s Chancellery, Office IIb, and Herbert Linden of Department IV of the Reich Ministry of the Interior did the recruiting. Once a doctor agreed to participate in the euthanasia program, he or she became an associate of the “Reich Committee” (Friedlander, 1994, pp. 48-49; M. Burleigh, 1994, p. 101).
At these children’s wards, the Führer’s Chancellery left it to their hand-selected physicians to devise efficient means of killing. Their preferred method was overdoses of medication. At Steinhof in Vienna, mentally disabled children were given excessive dosages of morphine-scopolamine; at Eglfing-Haar in Bavaria, they received lethal cocktails of luminal and veronal. The “medication” was administered either in tablets or in liquid form to the children. Occasionally, it was injected directly into them. From the standpoint of preserving secrecy, there was much to commend these medications as killing agents. First, they were readily available in German mental hospitals as sedatives. Second, they were not poisons, and became deadly only in overdoses. Third, they did not immediately kill the child; rather, they typically gave rise to complications like pneumonia, which then became the immediate cause of death after two or three days. The physician could then soberly ascribe the child’s death to a conventional cause, rather than to poisoning. Although the Führer’s Chancellery supplied the children’s wards with sufficient amounts of the medications, the Chancellery’s own supplier was Office V of the Reich Security Main Office (RSHA), the Criminal Police Office. From the time the children’s wards were established until the end of the war, the Criminal Police was the main provider to the Führer’s Chancellery of the medications used to kill both mentally ill children and adults (Friedlander, 1994, p. 54).
Clearly, this program required that the children identified by the medical experts of Hitler’s Chancellery for killing be transported to the children’s wards. The Chancellery did not itself arrange the transfer of the children to the wards; rather, this was left to individual state health offices within local ministries of the interior. Thus, for example. Business Section X of the Württemberg Ministry of the Interior, which administered mental institutions in the state of Baden-Württemberg, directed the transportation of 93 children from Württemberg institutions in late 1942 to the children’s ward at Eichberg, where they were murdered. The order to put the children to death, however, always originated with the central authorities at the Führer’s Chancellery, working through their front organization, the Reich Committee. The killing order arrived as an official document under the letterhead of the Reich Committee, bearing the signature of a Chancellery bureaucrat—frequently Hefelmann. The language of the order was couched in euphemisms: the word “treatment” functioned as a code word for killing (Rüter, 1968-1981, Serial Numbers 117a, 155a, 155b, 211).
German researchers vied for access to the bodies of the murdered children. Two research centers were particularly allied with the euthanasia program. The first was a data collection department attached to the killing center at Brandenburg-Görden (site of the first children’s ward) under the direction of a medical expert in the Führer’s Chancellery, Professor Hans Heinze; the second was the Clinic for Psychiatry and Neurology of Heidelberg University, led by Dr. Carl Schneider. These research centers (and others as well) studied the Reich Committee children before they were transported to pediatric wards for killing. On a routine basis, they autopsied the corpses of the children, removing organs from them (especially their brains) for subsequent analysis. At Görden, for example, 33 children were killed on October 28, 1940, and dissected for their brains within four hours of their death. These children, it should be emphasized, were not “mentally dead” creatures in continual pain; in fact, they attended a special school in Brandenburg-Gorden. Many of them came from underprivileged or abusive family backgrounds. These victims were far from beneficiaries of a “mercy death;” they were relatively healthy children, albeit disabled, responsive to their environment and capable of enjoying their lives— children murdered by the euthanasia doctors for the primary purpose of harvesting their bodies for research materials (Friedlander, 1994, pp. 58-59; Klee, 2001, p. 250; Aly, 1994, p. 224).1)
As in National Socialist killing projects generally, so in the children’s euthanasia program a tendency to break out of prescribed limits arose as the war progressed. The program began with newborns and children under the age of three; when military defeat had ended it in 1945, it had grown to include older children and teenagers. Nor were all of these youngsters “empty shells of human beings,” to use the frequently cited phrase of Binding and Hoche. Like the 33 children killed in October 1940 at Görden, not a few had been institutionalized for learning disabilities or adjustment disorders.
The incompleteness of the historical record makes a death toll impossible to determine with precision. The Frankfurt prosecutor’s indictment of Werner Heyde, Gerhard Bohne, and Hans Hefelmann in May 1962 estimated a figure of around 5,000 (Friedlander, 1994, p. 61).
The Adult “Euthanasia” Program, 1939-41
Children’s euthanasia was a prologue to the more ambitious and destructive campaign to kill mentally ill adults. Sometime in July 1939, Hitler commissioned his escort physician, Karl Brandt, and the head of the Führer’s Chancellery, Philip Bouhler, to organize adult “euthanasia.” In collaboration with Herbert Linden of the Reich Ministry of the Interior’s Department IV (a co-developer of the children’s program), they assembled a circle of ideologically reliable doctors around them to assist with planning and executing the program. The circle included the chaired professor of neurology and Psychiatry, Max de Crinis; the director of the Clinic for Psychiatry and Neurology of Heidelberg University, Carl Schneider; Professor Berthold Kihn of Jena; and Werner Heyde, Professor of Psychiatry and Neurology at the University of Würzburg. The circle of initiates also included Ernst Wentzler, Helmut Unger, Hans Heinze, Hermann Pfannmüller, Dr. Bender of the mental hospital at Berlin-Buch, and Professor Paul Nitsche of the asylum at Sonnenstein near Pirna. In late July and August 1939, a series of meetings occurred between these hand-selected individuals in Berlin. Bouhler explained to the participants that “euthanizing” mental patients in German asylums and nursing homes would create necessary hospital space for the impending war, freeing up medical staff to care for the wounded. Bouhler further indicated that Hitler had refrained from publishing a euthanasia law for foreign policy reasons. He went on to reassure everyone present that they would be immune from criminal prosecution for their actions in connection with the killing program, inviting dissenters to withdraw from involvement if they so desired. Bouhler’s invitation met with overwhelming acceptance. Bouhler then suggested that a system of expert evaluation should be created “similar to that envisioned in the work of Hoche and Binding” (Statement by Werner Heyde, qutd. in Klee, 1986, p. 84).
After the initial recruitment meeting with Bouhler in the summer of 1939, the physicians returned to their institutions and sought out suitable personnel there for the work of mass killing. The names of these individuals were then relayed to the Führer’s Chancellery in Berlin. In the meantime, having found accomplices for their murder project, Bouhler and Brack applied their ingenuity to choosing an appropriate means of killing. Wanting something that was quick, lethal, and painless, they consulted three prominent pharmacologists, who recommended the substance that would become the murder agent of choice in the first phase of Nazi euthanasia: carbon monoxide gas. A chemist in the Criminal Technical Institute (KTI) within the Reich Security Main Office, Dr. Albert Widmann, confirmed the pharmacologists’ recommendation in a meeting with Viktor Brack. Brack commissioned Widmann to obtain canisters of carbon monoxide and deliver them to the Führer’s Chancellery. Presumably, the aim here was to divert any possible suspicion away from the Chancellery by using another organization to procure the lethal materials. Widmann accepted this commission, and thereafter received orders for the poison from the individual killing centers, which he filled in the name of the KTI at the I.G. Farben factories in Ludwigshafen. A Chancellery official. Dr. August Becker, arranged for picking up and transporting the carbon monoxide canisters to the killing centers. All costs incidental to these orders were charged to the KTI (Klee, 1986, p. 84).
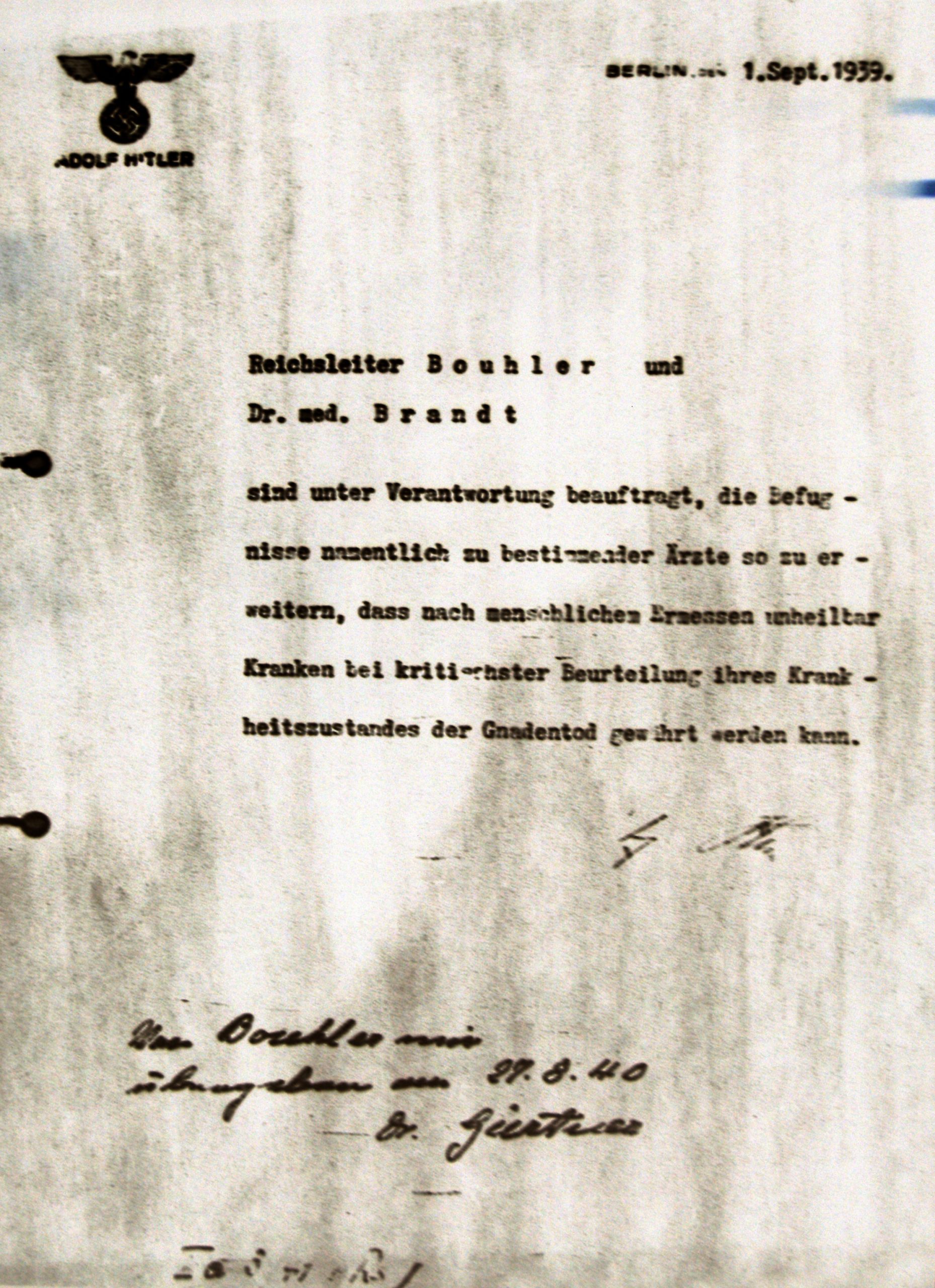
Concerns about the legality of the killing program nonetheless persisted. Under German law killing a human being—except for battle-field combat and the legal execution of persons duly convicted and sentenced by the courts—was a capital offense in Germany even during the Nazi era. At a meeting called by Hitler sometime in September 1939 to discuss the euthanasia program, the Chief of the Reich Chancellery and Hitler’s closest legal advisor, Hans Heinrich Lammers, argued that the program should be established on a legal basis. If Lammers’ testimony under U.S. Army interrogation is to be believed. Hitler commissioned Lammers with drafting a euthanasia law. The draft was accordingly prepared, but Hitler subsequently changed his mind, on the grounds that an official law would “cause too great a sensation” (Testimony of Hans The “euthanasia” authorization signed by Adolf Hitler and backdated to September 1, 1939. Source: Wikimedia, Heinrich Lammers, 1945, pp. 876-77). Throughout the duration of the killing program, many of the health care providers and public health officials involved in it would express their fears of criminal liability without an authorizing statute. Acting on their concerns, the Führer’s Chancellery asked Hitler for a written authorization for euthanasia. He assented, and the Chancellery prepared for his signature an authorizing document, printed on Hitler’s own stationery. He signed the authorization in October 1939 but backdated it to September 1, 1939. It read:
Berlin, 1 September 1939
Reich Leader Bouhler and Dr. med. Brandt are charged with the responsibility of enlarging the competence of certain physicians, designated by name, so that patients who, on the basis of human judgment, are considered incurable, can be granted mercy death after a critical evaluation of their state of health. (signed) A. Hitler (excerpted in Klee, 2001, p. 85)
Although Bouhler was in charge of the adult euthanasia program, he rarely participated in its daily operations. He entrusted the hands-on supervision of euthanasia to his deputy, the Chief of Section II of the Chancellery, Viktor Brack. Brack, whose educational background was not in medicine but in agriculture, sought to conceal the central role of the Führer’s Chancellery in “euthanasia” killing. From the beginning, it was understood that adult euthanasia would surpass in scope the relatively modest children’s program. It was therefore clear to Brack and his associates that their current offices in the Voss Strasse in Berlin would be inadequate to accommodate the enlarged staff needed to administer the program. Central Office II of the Führer s Chancellery thus relocated to a confiscated Jewish house at number 4, Tiergartenstrasse, in Berlin-Charlottenburg. This address lent its name to the central killing administration, which was thereafter referred to as “T4.” The T4 killing program itself was called “Operation T4” (Friedlander, 1991, p. 68).
“T4” (in reality, the Führer’s Chancellery, Main Office II) embraced numerous offices within its bureaucratic structure, as depicted in Table 2. These offices were the real powers behind a series of front organizations Chancellery officials to disguise its involvement in the program. Central to this operation was the T4 Medical Office, which evaluated registration forms, selected patients for killing, and both appointed and trained the medical staffs detailed to the killing centers.
In a children’s “euthanasia program” a single front organization, the Reich Committee, concealed the Chancellery’s involvement. Four such entities were established for the adult program: (1) the Reich Cooperative for State Hospitals and Nursing Homes; (2) the Charitable Foundation for Institutional Care; (3) the Central Accounting Office for State Hospitals and Nursing Homes; and (4) the Charitable Foundation for the Transport of Patients, Inc.
The Reich Cooperative for State Hospitals and Nursing Homes (RAG), a front for the T4 Medical Office, conducted correspondence with private and governmental parties about the process of registering, evaluating, and selecting adult patients for “euthanasia.” The Charitable Foundation for Institutional Care was a front for the T4 Central Office and dealt with all matters related to financing the program, including hiring and compensating employees of T4. The Central Accounting Office for State Hospitals and Nursing Homes collected payments for patient care. Its practice of charging per diem expenses for patients even after they had been liquidated enabled T4 to run consistently in the black, using the excess proceeds to finance its operations.
The Charitable Foundation for the Transport of Patients, Inc. (GEKRAT) camouflaged the T4 Transport Office; it transferred patients selected for euthanasia to the killing centers. The Reich Cooperative and GEKRAT were established in November 1939; the Charitable Foundation and the Central Accounting Office were erected in April 1940, coinciding with the Main Office II’s move into the Tiergartenstrasse villa (Friedlander, 1994, pp. 73-74; Klee, 2001, 93; Klee, 1986, 102-03).
| Office | Chief |
|---|---|
| Führer’s Chancellery Central Office II |
Viktor Brack Deputy: Werner Blankenburg |
| T4 Central Office |
Manager Gerhard Bohne Summer 1940: Dietrich Allers |
| T4 Medical Office |
Werner Heyde Dec. 1941: Paul Nitsche |
| T4 Medical Office |
Dec. 1941: Paul Nitsche |
| T4 Administrative Office |
Gerhard Bohne Summer 1940: Friedrich Tillmann |
| T4 Central Finance Office |
Willy Schneider March 1941: Fritz Schmiedel Jan. 1942: Friedrich Robert Lorent |
| T4 Transport Office |
Reinhold Vorberg Deputy: Gerhard Siebert |
| T4 Personnel Office |
Friedrich Hau Arnold Oels |
| T4 Inspector’s Office | Adolf Gustav Kaufmann |
As in the children’s program, so with adult euthanasia a decree by the Reich Ministry of the Interior facilitated the registration of patients targeted for destruction. On September 21, 1939, the Reich Ministry of the Interior dispatched a decree to state governmental offices called “The Registration of State Hospitals and Nursing Homes.” It required that local authorities supply the names of all mental hospitals within their region to the Reich Ministry by October 15, 1939, in which “mental patients, epileptics, and the feebleminded” were institutionalized. All institutions, public, private, religious, and charitable, were included, as were old-age homes. The Ministry of the Interior informed the respondent state authorities that the information was needed because the Ministry wished to send questionnaires directly to such institutions throughout Germany; local governments were to ensure timely completion and submission of the questionnaires.
Once the lists of institutions had been returned, the Reich Ministry sent the questionnaires to them, either directly or through the local state offices. The documents consisted of a single-page questionnaire that canvassed data about the size, staffing, and patient population of the institution. More ominously, it inquired about the number of patients with a criminal background, the number of Jewish patients, and the proximity of the institution to transportation arteries. In addition to the single-page questionnaire, the document package included a set of one-page reporting forms to be filled out by a doctor on individual patients. The form asked for the name, birth date, nationality, race, period of institutionalization, the names of relatives and frequency of their visits, the name and address of the guardian and the payor, and whether the patient had been institutionalized for criminal insanity. Finally, the doctor was invited to offer his diagnosis in a cramped section on the form and to evaluate the patient’s ability to perform work (Friedlander, 1994, pp. 75-76; Klee, 1986, pp. 87-88).
Attached to these forms was a one-page instruction sheet that identified the kinds of patients to be registered. These included patients who had been institutionalized for five years or longer; patients suffering from schizophrenia, epilepsy, senility, therapy-resistant paralysis and other syphilitic diseases, feeblemindedness, encephalitis, Huntington’s disease, and other terminal neurological diseases, so long as these patients were incapable of any work in the institution other than purely mechanical work (such as weeding); patients institutionalized for criminal insanity; or patients who were neither German citizens nor of German or related blood. For patients falling into the last category, the instruction sheet required the reporting doctors to describe the citizenship and race of the patient. In a footnote, the sheet provided examples: “German, or related blood (German-blooded), Jewish, Jewish hybrid (Mischling) of the first or second degree, Negro, Negro hybrid, Gypsy, Gypsy hybrid, etc.” (reproduced in Klee, 2001, p. 96).
As it did with the children’s program, the Führer’s Chancellery established a system of medical experts to review the incoming registration forms submitted from German mental hospitals. The system of expert review in the adult example, however, was more intricate than the children’s program. The Medical Office of Hitler’s Chancellery, Section II, in its guise as the Reich Cooperative for Mental Hospitals and Nursing Homes, established a two-tiered structure of expert review. The first tier consisted of medical experts, to whom the registration forms were first sent for evaluation. Their assessments were then proofed by a second tier of experts to guard against error. Some forty doctors, among them nine professors of medicine, served at one time or another as medical experts for T-4. Of this number, the overwhelming majority were first-tier experts. As the program unfolded, only three doctors— Werner Heyde, chief of the T4 Medical Office till December 1941, Paul Nitsche, Heyde’s successor, and Herbert Linden of the Reich Ministry of the Interior’s Department IV—would function as second-tier experts (Friedlander, 1994, p. 77).
When the registration forms arrived at the Reich Ministry. Herbert Linden sent them to the T4 Medical Office, where they were collated and catalogued. Five photocopies were made of the original forms; one copy was sent to each of three first-tier medical experts for evaluation. After a period of time the photocopies returned to the Medical Office, marked with one of three characters: a plus sign (+) in red meant that the patient was to be killed; a minus sign (—) in blue signified that the patient should be spared; and, occasionally, a question mark indicated a borderline case. A majority of the three first-tier experts determined whether a patient lived or died; unanimity was not required. Once the three photocopies with their annotations were collected, they went along with the original form and one more photocopy to the second- tier experts, typically Werner Heyde and Paul Nitsche. These top-level reviewers, in no way bound by the opinions of the first-tier experts, marked the additional photocopy with either a plus sign (death) or a minus sign (life). The second-tier experts were the ultimate judges of life and death for the registered patients, determining literally with the stroke of a pen who would be allowed to live and who would perish. If the form bore a plus sign, the T4 Medical Office sent it to the T4 Transport Office, which drafted lists of the patients designated for killing (Klee, 2001, 97-98; Friedlander, 1994, p. 83).
Several days prior to transport, the T4 Medical Office contacted the institutions that accommodated the selected patients. (Notice was conveyed via Linden’s Department IV in the Reich Ministry of the Interior to individual state interior ministries, and thence disseminated to local mental hospitals.) These institutions were instructed to send all medical records and personnel files along with the patients, as well as all their personal possessions (money, jewelry, etc.), which were to be logged on special forms. Prior to the pickup day, the T4 Transportation Office (GEKRAT) sent a list to the surrendering institution of the patients to be transported. Perhaps as a result of the doctors’ intentional practice of underestimating their patients’ capacity for work, perhaps due to the haste with which the forms were reviewed by the T4 experts, GEKRAT’s lists often contained the names of patients who did productive work in the institution. In such cases, institutional directors tried to persuade the GEKRAT representatives to exempt these patients from transport. Since a sum-certain quota of transportées had to be filled, GEKRAT typically agreed to exemption only if other patients could be substituted. The patients appearing on the final GEKRAT list were picked up in large gray busses. Occasionally, some patients among those transferred seemed to intuit what was happening, and scenes of crying, pleading, and protest broke out as they were forced into the busses (Friedlander, 1994, pp. 83-84; Klee, 1986, pp. 124-30).
Once the patients had left the surrendering institution, it notified the next of kin that the patient had been transferred to another facility on orders of the Reich defense commissar, and that this facility would eventually contact them about their relative. Within a brief span of time, the killing center wrote to them that the patient had arrived, but it forbade them from visiting their relative with the assurance that they would be apprised of any change in his or her condition. In reality, the killing center— like so many of the T4 individuals, offices, and institutions— imitated a conventional mental hospital as part of the charade to deceive onlookers. When the patient was killed, the killing center authorities informed the family of the death, ascribing it to natural causes and reporting that the risk of epidemic disease had forced the institution to cremate the body. An urn containing the ashes was available for shipment to them (Friedlander, 1994, p. 85).
The T4 Killing Centers
The idea of establishing killing centers developed out of discussions between representatives of Hitler’s Chancellery, the Reich Ministry of the Interior, and the chemist Albert Widmann of the Criminal Technical Institute (KTI) in the Reich Security Main Office. Widmann later testified that Leonardo Conti, the Reich Health Leader and head of the Department of Health in the Ministry of the Interior, had rejected injections as a killing agent in favor of poisonous gas. As we have seen, in the aftermath of these discussions, Widmann met with Viktor Brack to work out the mechanics of how the patients would be gassed. Widmann’s suggestion that carbon monoxide gas be released through the air ducts of the patients’ hospital rooms was dismissed on practical grounds. The notion of the killing center emerged as a more practical alternative (Testimony of Albert Widmann, 1960, cited in Friedlander, 1994, 86-87).
Brack and Karl Brandt had a short-lived difference of opinion about the most effective way to kill the patients. From his discussions with Widmann, Brack was convinced of the utility of carbon monoxide. Brandt, however, initially opposed this idea, countering that, since the euthanasia program involved “medical measures,” a “medical means” must be adopted; he favored lethal injections. (Brandt eventually overcame his scruples and agreed on carbon monoxide.) Postwar forensic testimony by ex-T4 leaders indicates that the decision to test the effect of carbon monoxide gas on human guinea pigs grew out of this disagreement between Brack and Brandt (Testimony of Gerhard Bohne, 1959, qutd. in Klee, 1986, p. 110).

The experiment took place sometime in the early winter of 1939-1940 at Brandenburg an der Havel, a former jailhouse in the city of Brandenburg conveniently linked to Berlin by rail. Workers from the SS Main Construction Office installed in this vacated prison something that would become an infamous symbol of Nazi genocide—a gas chamber disguised as a shower room. The KTI’s own Dr. Widmann conducted the first gassing (an assertion Widmann strongly denied after the war). Also present at the demonstration was a Who’s Who of T4 leaders: Richard von Hegener and Hans Hefelmann of Office II b of Hitler’s Chancellery; Dr. Irmfried Eberl, director of the killing centers at Brandenburg and Bemburg before appointment as commandant of Treblinka; Dr. Ernst Baumhardt, director of the killing centers at Grafeneck and Hadamar; Karl Brandt and Philip Bouhler; Reinhold Vorberg, the chief of the T4 Transport Office (GEKRAT); Leonardo Conti and Herbert Linden; Viktor Brack and his deputy, Werner Blankenburg; Werner Heyde and Paul Nitsche of the T4 Medical Office; and Christian Wirth, who became involved in mass gassings of patients at Grafeneck, Brandenburg, Hadamar and Hartheim en route to his work as commandant at the death camps of Belzec, Sobibor, and Treblinka (Klee, 1986, p. 111; Friedlander, 1994, p. 87; Klee, 2001, pp. 20-21).
An eyewitness described after the war the spectacle that these euthanasia luminaries had gathered to view:
… around 18 to 20 people were led into this “shower room” by nursing staff. These men had to undress in the antechamber, so that they were completely naked. The doors were closed behind them. These people went into the room quietly and with no signs of agitation. Dr. Widmann operated the gassing equipment. Through the viewing window I could see that after a few minutes the patients keeled over or lay down on the benches. There weren’t any kind of scenes or tumults. After another 5 minutes the room was aired out. SS people designated for the task removed the dead from the room on specially-constructed stretchers and brought them to the cremation ovens. If I say specially-constructed stretchers, I mean stretchers constructed just for this purpose. These could be set directly in front of the cremation ovens and by means of a device the corpses could be mechanically conveyed into the ovens without the need for the carrier to touch the corpse. These ovens and stretchers were built in Brack’s office (excerpted in Klee, 1986, p. 111).
During this same period at Brandenburg, six mentally disabled patients were given lethal injections of morphine and scopolamine by Brandt and Conti. The purpose of the injections was to compare their effectiveness with carbon monoxide. According to Werner Heyde. our primary source for this episode, the results cast doubt on the injection method: “The patients,” Heyde remembered, “died quite slowly, and it is possible . . . that the injections had to be repeated.” According to one postwar eyewitness, Brack was “satisfied” with the carbon monoxide experiment. Even Brandt was won over to carbon monoxide, but stressed along with Brack that “these gassings should only be performed by doctors.” “In this way,” the eyewitness summed up, “the beginning [of gassings] in Brandenburg was deemed a success” (qutd. in Klee, 1986, p. 111).
Brandenburg became the first of six institutions specifically designed to kill “unworthy life” with carbon monoxide gas. Shortly after Brandenburg became operative, Grafeneck in Württemberg opened its doors in January 1940. To deal with the volume of victims, T4 opened two other killing centers at Hartheim near Linz (May 1940) and Sonnenstein in Pirna near Dresden (June 1940). The final two euthanasia centers, Bernburg on the Saale River and Hadamar just north of Wiesbaden in Hessen, were designed as successor institutions to Brandenburg and Grafeneck. In each of these killing centers, a suitable room was chosen for conversion into a gas chamber disguised as a shower room. The design in all material respects followed the model of Brandenburg. Moreover, jurisdiction over killing was divided among each of the institutions. Brandenburg killed mental patients from Berlin, the Prussian provinces of Brandenburg, Saxony, and Schleswig Holstein, and the states of Brunswick, Mecklenburg, Anhalt, and Hamburg. (As Brandenburg’s successor, Bernburg would cover this region after 1941.) Grafeneck disposed of south German patients from Bavaria, Württemberg, and Baden; its own successor, Hadamar, took over these regions plus the state of Hessen and the Prussian province of Hanover. Hartheim killed patients from Austrian mental institutions, as well as some from southern Germany and Saxony. Finally, Sonnenstein gassed patients from Saxony, Thuringia, Silesia, and southern Germany (Friedlander, 1994, p. 93).
“The subterfuge developed by the killing center staffs to deceive the patients was the appearance of normality,” Henry Friedlander has written. “Every procedure was designed to conceal the function of the killing center and to simulate a normal hospital” (Friedlander, 1994, p. 94). The appearance of normality misled the patients into the belief that they were being transferred to a hospital no different from other institutions already familiar to them. GEKRAT buses transported the patients to the killing center. In some cases, they arrived by rail and were then picked up by so-called “death buses” that drove them to the institution. Upon arrival, patients were met by staff members who conducted them to a changing room, where they were instructed to remove their clothes. The postwar testimony of a Hadamar nurse illustrates the procedure observed in all the killing centers:
. . . On the ground floor, the victims came into a reception area divided at the time into two rooms, the first of which served as a waiting area. Here some beds were provided for non-ambulatory patients. The second room of the reception area was the changing room, in which I was involved. There first the men and then the women were disrobed. From here, the patients were led through a hallway into the doctor’s room, where they were again given a brief medical exam and were given a number with reference to their medical papers. These numbers were written on their backs with a colored marker. From the doctor’s room they came into an adjacent room, the purpose of which I do not know. From this room they were led into a photography room next door, in which they had to wait until all the members of the transport had been gathered. They were then brought together down a staircase into the gas chamber lined with glazed tiles, which outwardly resembled a shower (Statement by Nurse Isabella W., 1946, excerpted in Klee, 2001, p. 119).
The “brief medical exam” mentioned by this nurse was alleged by T4 defendants to ensure that only incurable and severely ill patients were earmarked for killing. In a rare moment of candor, however, a T4 doctor admitted after the war that these exams were performed in order to find the most plausible “cause” of death for entry on the patient’s death certificate. “The persons were led to us, that is either to me or to Dr. Eberl or both together,” the doctor recalled. “We examined the patients and then determined what cause of death could be used. We then entered the cause of death in the space on the lower left [of the registration form]. . . . They were led from our room directly into the so-called shower rooms, in order to be put to sleep there with carbon monoxide gas” (qutd. in Klee, 2001, p. 124).
At least some of the patients he observed by one postwar witness “still had a certain mental ability,” as evidenced by the fact that they carried washcloths and soap with them into the gas chamber (Statement of Vinzenz Nohel, 1945, excerpted in Klee, 2001, p. 124). When the patients had all entered the gas chamber, the gassing technicians ensured that the door and ventilation shafts were tightly sealed. Only then did the physician open the valve of the gas tank and fill the chamber with carbon monoxide. Within five minutes, all the patients were unconscious; within ten, they were dead. Staff members waited a couple of hours before airing out the chamber with fans. Once this had been done, attending physicians pronounced the victims dead and the corpses were carried out (or, in some instances, dragged out) by the stokers to a nearby room, where the bodies were arranged in piles. The bodies were done one final indignity before cremation: they were plundered by staff members. Patients with gold teeth had been marked prior to gassing with a cross on their backs (at Sonnenstein, the marking was on their chest). A staff member identified the corpses with gold teeth by these markings and wrenched the teeth out of their mouths with pliers. They were deposited with a secretary in the institution’s main office, and eventually forwarded to the T4 authorities in Berlin. Other corpses became the objects of autopsies, designed both to train younger physicians (who received academic credit from the autopsies) and to harvest brains for study in German research institutes (Friedlander, 1994, p. 97).
The stokers cremated the bodies of the murdered patients in ovens, working in shifts through the night to reduce the corpses to ashes. The ashes were literally swept into a pile and indiscriminately deposited in urns. Each um bore the name of a patient killed in the gas chamber, but it did not necessarily contain that patient’s ashes. The names of each patient were then entered in the death book maintained at every killing center. Obviously, the T4 killers could not report that a large number of patients (some transports comprised as many as 150) had all died simultaneously of natural causes. False causes and dates of death had to be concocted. At the beginning of the euthanasia program, the T4 Medical Office disseminated lists of “causes of death” to its participating doctors that could be cited in furtherance of the charade. One such list contained 61 different illnesses, along with brief descriptions of the etiology (cause), course (symptoms, duration, fever, differential diagnoses), therapy, and complications of each disease. Stroke, pneumonia, heart attack, tuberculosis, and circulatory collapse were among the causes of death most frequently given. The killing center doctor recorded the fraudulent cause of death on the death certificate, certifying it with a false name, and this fiction was reproduced in official correspondence and in so-called “consolation letters” sent to the patient’s family or guardian. Since the patient had already been gassed before the killing center’s notification of his or her safe arrival had been sent to the relatives, it was likewise necessary to falsify the date of death. The administrative offices of the killing centers sent the “letter of consolation” to the family or guardian around ten days after the patient’s death. The letter was boiler plate, informing the family of the patient’s death and the “cause” and “date” of his or her demise, and offering an unctuous reassurance that the patient had been “delivered” from suffering. It also indicated that, in order to “hinder the outbreak and spread of communicable diseases,” the local police authorities had required the cremation of the patient’s body and the “disinfection” of his or her belongings. Urns containing the ashes would be sent to the family if they
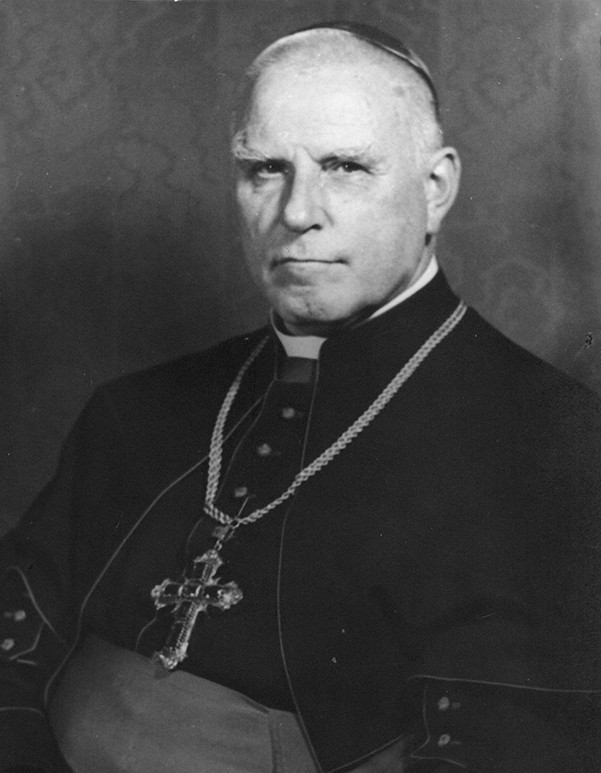
responded within 14 days and presented proof that they had made arrangements for proper interment (Friedlander, 1994, pp. 98-101; Klee, 2001, pp. 139-40; Klee, 1986, pp. 149-53).
By August of 1941, the death toll of mentally disabled patients murdered in T4’s killing centers had reached 70,273. These figures are based on numbers compiled by a T4 statistician discovered at the Hartheim institution after the war. German prosecutors after the war, however, believed these figures underestimated the number of the dead. Based on the evidence they had collected, they argued the T4 statistician had, among other miscalculations, miscounted the patients “euthanized” at Hartheim and Sonnenstein. They arrived at a conservative estimate of 80,000 patients killed until the official “end” Of the operation in August 1941 (Friedlander, 1994, p. 110; Klee, 2001, pp. 340-41).
We do not know for certain why Hitler ended the first phase of adult euthanasia on August 24, 1941. The likely explanation is pressure from the Catholic church. The bombshell was a sermon delivered on August 3, 1941, by Count Clemens August von Galen, the bishop of Münster. Galen was informed in July 1940 that Leonardo Conti’s ministry (Department IV of the Interior Ministry) had authorized a program of euthanasia against the mentally disabled. Galen and his associates chose not to lodge a public protest at that time, however, for lack of sufficient evidence. By August of 1941, Galen felt it was time to go public; his sermon represented the first public protest against Nazi euthanasia. In the sermon, Galen referred to the high mortality rate among the mentally ill in German institutions that “did not occur randomly, but rather was intentionally produced.” He condemned the killings as violations of German homicide law and of the 5th Commandment, “Thou Shalt not Kill” (Sermon of Bishop Galen, 1941, reproduced in Klee, 2001, pp. 193-98). Galen’s sermon was read from pulpits throughout his diocese, and soon became a topic of discussion both within and outside Germany. (British pilots dropped thousands of copies of the sermon on German cities.)
The Nazi elite was furious. A propaganda director, Walter Tiessler, suggested to Bormann that Galen be hanged. The proposal was rejected on the grounds that executing Galen would only turn him into a “martyr” and stir up even more popular unrest. In the meantime, Galen’s sermon had opened the floodgates to protests from Catholic and Protestant clerics, many of which were sent directly to the National Socialist leadership (Klee, 2001, p. 336).
On August 24, 1941, in the face of mounting pressure from the church and public unrest, Adolf Hitler ordered an official cessation to the euthanasia program. Notwithstanding this order, however, the murder of mentally disabled patients continued in T4 killing centers, with one critical difference: whereas the pre-August 1941 T4 killings were restricted to psychiatric patients, the radius of killing after the August stoppage was expanded to new categories of “unworthy life,” defined less in medical than in social, racial, and political terms.
“Wild” Euthanasia, September 1941-April 1945
Even after the euthanasia “stop,” the Reich Ministry continued to distribute questionnaires to German mental institutions biannually. In his role as Reich Commissioner for Mental Hospitals, Herbert Linden submitted the forms to Hitler’s Chancellery medical experts for evaluation. Killing proceeded on the basis of these expert assessments, but the gas chambers of the killing centers were largely dismantled; henceforth, patients selected for euthanasia were given lethal overdoses or injections of narcotics, or simply starved to death. Furthermore, while original killing centers like Hadamar and Bernburg were still euthanizing patients after the stop order, the focus of killing shifted to the transit centers— many of which were simultaneously murdering disabled children in their children’s wards. Facilities such as Eichberg, Kalmenhof, and Eglfing-Haar began to kill adult patients on-site. The Meseritz-Obrawalde mental hospital in Pomerania and Tiegenhof (Dziekanka) in the Wartheland became major centers for destroying the mentally handicapped. These institutions represent only a fraction of the facilities involved in killing the disabled during the period of “wild” euthanasia that ensued after August 24, 1941. A considerable number of hospitals murdered their patients when transportation to defunct killing centers became impossible (Friedlander, 1994, p. 152).
The key point here is that the T4 Offices continued to register and evaluate patients for killing even after the official “stop;” it never fully relinquished control over euthanasia to local institutions. Just as it had up to August 24, the T4 authorities in Berlin directed the transports of patients to destinations where they were killed, provided these facilities with narcotics to poison them, and made available its experienced personnel to perform the killings. Nonetheless, T-4’s control of euthanasia was not as top-down as it had been during Phase 1, when the T4 Central Office had orchestrated a program of selection, transportation, and immediate killing on arrival at one of the six killing centers. Phase 2 (“wild”) euthanasia transpired in numerous institutions, the sheer number of which posed obstacles of command and control to the Berlin offices (Klee, 1986, p 441; Friedlander, 1994, p. 155).
The period of “wild” euthanasia also saw intense aerial bombardment of German cities and production centers by the Allies. The result of Allied bombing was a grave crisis in hospital space to accommodate the wounded. Already in 1941, Hitler had ordered Karl Brandt “to designate evacuation hospitals for other cities that were in danger.” On July 28, 1942, Hitler appointed Brandt “Commissioner for the Health Care System,” in which capacity he developed an official program code-named “Operation Brandt.” Under its auspices, mentally disabled patients were evacuated from psychiatric hospitals and clinics. The reason offered for their removal was to protect them from air raids. Even as the authorities professed a concern for their safety, these same patients were transferred to institutions in the occupied territories like Meseritz-Obrawalde or to Reich facilities such as Hadamar, Eichberg, and Kaufbeuren, where physicians and nurses killed them through starvation or overdoses of medication. The surrendering institutions themselves, rather than the T4 experts in Berlin, typically chose patients for transport. The language in the evacuation orders was calculated to mislead both the public and the surrendering institutions into believing that the transfers were undertaken in the patients’ interests. After the war, a T4 official involved in the evacuations admitted that exposure to bombing was a non-factor in the transports. In this manner, in early 1943 hundreds of patients were transferred from mental hospitals in the Rhineland to the General Government’s Kulparkov Asylum near Lvov and Warsaw’s Tvorki Asylum— thinly disguised killing centers for the mentally handicapped, in which all of these Rhineland patients died within one-and-a-half years (Aly, 1994, p. 84; Klee, 2001, p. 284).
Many other disabled patients met the same fate during Operation Brandt. In 1943, Brandt carved out hospital space by evacuating the “Mahaneim” house in Bethel and transferring the patients to the Meseritz-Obrawalde asylum for killing. When the mental hospital in Bremen was damaged during an air raid in November 1943, Herbert Linden invited the Bremen director to transfer some of his patients to Meseritz-Obrawalde. Of the 341 patients sent there, one died en route; by February 2, 1944, 242 others were dead (Aly, 1994, pp. 84-85).
With Operation Brandt, National Socialist euthanasia branched outward from allegedly “incurable” mental patients to embrace a variety of victim groups. As the war ground on, creating new problems for the German government within the Reich, the Nazis employed mass killing as an instrument of population policy. In the aftermath of the Hamburg incendiary bombings in late July 1943, for example, Hamburg women deranged by the trauma of the firestorm were transported to Hadamar, where it is believed they were all murdered. In addition to traumatized civilians, members of old-age homes became victims of Operation Brandt after the July bombing of Hamburg. They were transported to Neuruppin Mental Hospital and to Meseritz-Obrawalde for killing (Aly, 1994, pp. 86-7).
Eugenics in Nazi-occupied Eastern Europe
Before the T4 killing program had even started, the SS and the Gestapo were murdering mental patients in occupied Poland. Possibly at the suggestion of Gauleiter Schwede-Coburg, the president of Pomerania (the Prussian province on the Polish border), Heinrich Himmier decided after the invasion of Poland in September 1939 to clear Pomeranian nursing homes for use as SS military bases and field hospitals. The modus operandi consisted of shooting and gassing by mobile gas vans of allegedly “incurable” patients. The earliest mass murder of the mentally disabled occurred at the hands of SS troops in October 1939— nearly three months before the experimental gassing at Brandenburg. SS-Oberführer Kurt Eimann received the “unpleasant task” to clear Pomeranian mental hospitals on Himmier’s orders. The patients were to be “eliminated” so that these buildings could be used to care for wounded SS soldiers. There was no question in Eimann’s mind that “eliminated” meant “killed.” Vehicles belonging to the Danzig traffic police would transport the patients from the train station in Neustadt to the killing fields. Polish prisoners from the nearby concentration camp Stutthoff who had been sentenced to death were forced to dig mass graves for disposal of the corpses; afterward, Eimann’s men shot these prisoners. Eimann himself chose the site for the killing, a forested area near Piasnitz. The locale was ideal, since it was easily accessible to the Danzig police vehicles and afforded privacy against would-be eyewitnesses. This killing field was part of the Polish territory incorporated into the German Reich as the Reichsgau West Prussia (Statement by Kurt Eimann, 1968, excerpted in Klee, 2001, pp. 71-72).
As shooters and cordon guards Eimann selected members of his unit who had proven themselves “characterologically and ideologically reliable.” Sworn to secrecy prior to the operation, they were subjected to propaganda films and other morale-boosting measures so long as they participated in the killing. These individuals escorted the patients one by one from the vehicles to the trench; Eimann followed a short distance away. Once the patients had come abreast of the trench, one of the SS men shot them in the back of the neck, killing them instantly. (Eimann shot the first patient, a woman, in order to prove he was willing “to dirty his own hands” with the killing.) Their lifeless bodies crumpled into the mass grave. When the SS guards waiting at the vehicle parked fifty meters away heard the pistol shot, they prepared the next patient for the death march to the gravesite. The shooting continued for several hours until every patient had been killed. If a body in the grave exhibited signs of life, the SS killer shot him or her from the edge of the grave (Klee, 2001 pp. 71-72).
These shootings of Pomeranian and West Prussian mental patients lasted until the end of November 1939, amassing a death toll of around 3,500. Once the job was completed, Eimann and his men killed all the Stutthof prisoners (Friedlander, 1994, p. 137).
This destruction of disabled patients in Pomerania was only the beginning of a campaign of murder in the East that continued long after Eimann had finished his deadly errand. A ghastly episode of mass shooting occurred at the psychiatric hospital in Chelm Lubelski on January 12, 1940, where 440 mentally disabled patients were machine-gunned on the hospital grounds. The Chelm Lubelski shootings are described in the “Bulletin of the Main Commission for the Investigation of German Crimes in Poland:”
In the first days of January 1940, some Gestapo officers arrived…who were well acquainted with the terrain of the hospital and the patient lists. After a few days, on 12 January 1940,30 Gestapo soldiers arrived during the morning hours…, however, they did not reveal the purpose of their visit. At the same time, the Polish workers of a nearby brickworks were ordered to excavate two large trenches at a distance of 150 meters from the. hospital. That afternoon, the service personnel were all ordered to assemble in a special room, and after a few hours were ordered to leave the hospital premises. In the evening, the soldiers expelled the patients from Building 2. A machine gun was set up in front of the exit and opened fire on the patients as they were driven out of the hall over the threshold. A growing stack of corpses piled up. The resistant German patients were driven through the rooms and hurled out of the second or third floor windows. One young girl in particular, who suffered from psychotic depression, was hunted by the Germans throughout the entire building from floor to floor; finally she was found and thrown out a window on the second floor, and thereafter shot….
A few patients succeeded in breaking through the cordon of Germans, and thus began a hunt on the hospital grounds that ended with the murder of the runaways. A wounded patient fled almost a kilometer before he was captured and murdered. After a flight of three-quarters of a kilometer from the hospital, a second patient hid himself for almost a month before he was found and murdered….
The most difficult task for the Germans was seizing the children—patients in the pediatrics ward— who ran around on all floors and hid themselves in cabinets and under beds and the like. All the children were sought after and shot.
The pile of corpses was guarded by the Germans during the night. The moaning of the dying could be heard, because not all the victims had been killed; many of them had only been severely wounded.
Toward morning, the Germans halted the flow of farmers’ vehicles, sent the drivers home and ordered workers from the brickworks to load the corpses on the vehicles. The corpses were buried in two trenches, which had already been excavated. After the corpses had been removed, it was discovered that a patient who had lain at the bottom of the pile of corpses was still alive. When this patient crawled out and began to run away, she was shot…. (excerpted in Klee, 1986, pp. 114-15)
The shootings at Chelm-Lubelski were only a fraction of the murders committed against mental patients in occupied Poland during the war. Victims ranged from Pomeranian Germans, West Prussian Germans and Poles, and German, Jewish, and Polish mentally disabled patients from the Warthegau. The killers were typically members of the SS and Gestapo, although in at least one case German army soldiers carried out the shootings. Sometimes they acted in collaboration with German doctors. In the liquidation of mental patients at the mental hospital Kochanowka (Woiwodschaft Lodz) in March 1940, two German doctors, Herbert Grohmann and a Dr. Kleebank, selected patients for shooting. Similarly, at the psychiatric hospital in Wartha in April 1940, Dr. Fritz Lemberger and Hans Renfranz assisted the SS in killing 499 mental patients (Klee, 2001, pp. 72-73).
Pistols and machine guns were not the only weapons used against the mentally ill in Poland. Early on in these killings, another lethal device was deployed against them, the mobile gas van. This device was built in the summer of 1938 at the Sachsenhausen concentration camp and subsequently used to gas the mentally ill in Stralsund (Pomerania) and Posen (a German province lost to Germany after 1918 and reincorporated into the Reich as part of the Wartheland in the aftermath of the Polish campaign). The gas vans were essentially mobile gas chambers, often disguised as Kaiser Coffee Company delivery trucks. Patients were loaded into the sealed cab; attached to it with a rubber hose was a steel tank of carbon monoxide gas. The driver cranked open a valve on the tank, admitting pure carbon monoxide into the cab via the hose. Among the first “applications” of this technology was the clearing of the mental hospital Tiegenhof (Polish Dziekanka) near Gnesen in December 1939-January 1940. A unit specially created to kill Wartheland patients conducted the gassings, the Lange Commando under the direction of SS Captain Herbert Lange. The Commando arrived at the institution in early December 1939 and, after dismissing a large number of the nursing staff, loaded the patients in groups of ten into the gas van, in which they were asphyxiated
The T4 link with the Final Solution:
T4 officials became leaders in the genocide of European Jews


as it departed the hospital. The Polish doctor Jan Callus estimated the number of those murdered in this fashion between December 12,1939 and January 12, 1940 at 1,043 patients. The success of the Tiegenhof gassings, coupled with the favorable results of Viktor Brack’s experimental gassings at Brandenburg, convinced the Nazi authorities that carbon monoxide gas should be used as a killing agent to deal with the Wartheland’s mental patients (Aly, 1999, p. 71; Friedlander, 1994, pp. 137-38; Klee, 2001, p. 80; Klee, 1986, p. 113).
In January 1940, 534 patients of the Kosten mental hospital (Koscian/ Woiwodschaft Posen) were gassed over several days in vehicles disguised as furniture trucks. A few months later, in May and June 1940, the Lange Kommando was sent to the Soldau concentration camp in East Prussia to assist in killing German mental patients. At Soldau, the unit killed 1,558 patients in its gas vans in 19 days. Typically, it loaded on average forty patients into a van and gassed them as the vehicle drove away, dumping the bodies in mass graves in the lonely region around the Soldau camp. When the van returned after three hours, it was empty (Friedlander, 1994, p. 140).
The mass murder of patients in the eastern territories prior to the invasion of Russia was only tenuously related to the T4 program administered from Berlin by the Führer’s Chancellery. There were no registration forms, no expert evaluators, no T4 authorizations, no “mercy deaths’’ administered by medical personnel. Although in a couple of isolated cases German physicians participated in selecting patients for killing (as in the liquidation of patients at the psychiatric hospitals in Kochanowka and Warta), most of the selection and shooting were done by non-medical SS and Gestapo units. As the example of Chelm-Lubelski graphically proves, there was no pretense of ending the lives of suffering patients on humanitarian grounds in these killings— nor is any such pretense even maintainable. The SS needed hospital space and medical staff, and the mentally disabled were perceived as standing between the SS and the object it coveted. As the US Holocaust Memorial Museum webpage on T4 explains, “These murders [of the disabled in the east] lacked the ideological component attributed to the centralized Euthanasia Program” (United States Holocaust Memorial Museum, “Euthanasia Program and Aktion T4”). While this statement is undoubtedly true, it should be qualified. The ideology of “life unworthy of life” as it developed and spread through German society in the 1920s and ‘30s hardened the hearts and poisoned the minds of the SS against devalued populations like the disabled.
The United States Holocaust Memorial Museum, USHMM, website might be guilty of overstatement when it portrays the destruction of the disabled in Nazi Germany and the occupied territories as a “rehearsal” for later genocidal policies. “Rehearsal” suggests deliberation, a tuning up for the main event, and no proof exists that the Nazis in the late 1930s regarded T4 as a preparation for the Final Solution. Nonetheless, there is a clear throughway from sterilization, the children’s program, and adult euthanasia to the expanded killing programs of the Third Reich. Not least of the T4 program’s contributions to the Final Solution was the training of novices in mass murder. Gaining knowledge and experience in T4 between 1939 and 1941, they subsequently applied their savoir-faire to the genocide of the Jews, Roma, and other groups. T4 was well-represented among the staff assigned to the death camps of “Operation Reinhard” (the genocide of the Jews resident in the General Government). Among these crossovers were Franz Stangl (commandant of Treblinka and first commandant of Sobibor), Christian Wirth (first commandant of Belzec), and Irmfried Eberl (first commandant of Treblinka).
The final death toll of the Nazi “euthanasia” program in its two primary phases is not known for certain. Historians have cited figures from 250,000 to 300,000 victims.
Medical Ethics and Nazi Eugenics
The prostitution of medical science to Nazi ideology, like a meteor striking the surface of a planet, has left an indelible crater in ethical approaches to health care and scientific research. The most important judicial reckoning with Nazi medical criminality was the 1946 American Doctors Trial held in Nuremberg, Germany, which prosecuted twenty-three former members of the Nazi medical establishment. Although the accused were charged with involvement in involuntary sterilization, euthanasia, and criminal medical experimentation, the focus of the trial was clearly on the gruesome experiments conducted in German concentration camps. In its verdict delivered on August 20, 1947, the judges set forth a set of principles to determine when medical experimentation and treatment were permissible. The main criterion was “the voluntary consent of the human subject.” All together the court expounded ten principles to govern future medical experiments across the world (USHMM, “The Nuremberg Code”). These ten principles, which have since become known as the “Nuremberg Code,” are today regarded as international customary law (that is, applicable regardless of local law across the world).
10 Principles of the Nuremberg Code governing permissible medical experiments
- The voluntary consent of the humn subject is absolutely essential.
- The experiment should yield fruitful results for the good of society.
- The anticipated results must justify the performance of the experiment.
- The experiment must avoid all unnecessary suffering.
- No experiment should be conducted that leads to death or disabling injury.
- The degree of risk to be taken should never exceed that determined by the humanitarian importance of the problem to be solved by the experiment.
- Preparations should be made to protect the subject against death, injury, or disability.
- The experiment should be conducted only by scientifically qualified persons.
- During the experiment the human subject should be at liberty to bring the experiment to an end if he has reached the physical or mental state where continuation of the experiment seems to him to be impossible.
- During the experiment the scientist in charge must be prepared to terminate the experiment if he has probable cause to believe that a continuation of the experiment is likely to result in injury, disability, or death to the experimental subject.
Source: United States Holocaust Memorial Museum, 2022.
As for euthanasia since 1945, the Nazi experience has not deterred governments from passing laws to enable a “good death.” Some US states have permitted physicians to assist patients to commit suicide via “death with dignity” statutes. These include California, Oregon, Colorado, Vermont, Washington, and Washington D.C. Other legislatures, such as in Montana and Canada, have permitted physician-assisted suicide in terminal cases through the rulings of authoritative courts. Canada’s euthanasia law, with one eye trained on the Doctors Trial, allows assisted suicide only when the patient has given voluntary and informed consent to the procedure. Some countries have enabled medically-aided euthanasia for patients seeking release from mental illness (the Netherlands, Belgium, and Switzerland). Additionally, the Belgians permit patients by means of advance directives to give prior consent to euthanasia (Grodin et al., 2018, p. 56).
Like euthanasia, the legacy of eugenics left to posterity by Nazism is a cautionary tale for 21st century people. The Nazis sought to create a “master race” through promoting reproduction of allegedly valuable Germans while preventing by means of sterilization or mass murder the biological continuance of unwanted populations. Scientific advancements in genome editing have placed in human hands the ability to select for desirable traits in their children. The prospect of “designer babies” is no longer mere science fiction. Gene editing tools like CRISPR-Cas9 now allows for the alteration, addition, or removal of DNA sequences. This technology confronts us with a Janus face. On the one hand, most people would have few scruples concerning genetic interventions to avoid crippling, painful, or fatal illnesses. On the other, many would object to interventions to change the embryo’s eye or hair color, height, morphology, and other physical or mental traits, particularly when guided by the parents’ aesthetic preferences. In such cases, and in contrast with Nazi eugenics, the pressure to select for aesthetic characteristics emanates from private preference rather than government coercion. This difference aside, creating designer babies with qualities determined by the fads of pop culture is disturbing for many observers.
Gene editing is a decidedly ambiguous kind of eugenics. It occupies a liminal spot between positive eugenics (seeking to improve health and well-being, for example by curing or preventing disease) and negative eugenics (seeking to prevent certain kinds of human beings from existing or being born). Sterilization in the postwar world has tended more toward the negative side. As recently as the first two decades of the 21st century, 144 women prisoners in the California prison system were sterilized without their legal consent. After the sterilizations were publicized, California passed a law forbidding the sterilization of inmates within California prisons if done for reasons of birth control. The law also set forth the conditions under which legitimate sterilizations could be performed and mandated that all sterilizations be reported (Grodin et al, 2018, p. 56).
Conclusion
Underlying Nazi eugenics was the belief—not unique to Nazism—that individuals and groups had social value determined by their biology, and that the state should take steps to foster the reproduction of the valuable and deter or eliminate procreation of the inferior. This central tenet of Nazi eugenics should be the main criterion guiding our use of the Nazi analogy when analyzing eugenic actions by government or private persons today. Neither sterilization nor euthanasia are inherently linked to Nazism. The conscious, informed, and consensual decision of a patient to undergo either sterilization or euthanasia must be distinguished from Nazi practice. In the first, the decision is made freely by the person as an exercise of personal autonomy. The dignity of patients and their freedom to determine their own lives are respected. In the second, the decision-maker was a state authority hostile toward the well-being of the patient, motivated by a racist and crassly utilitarian view of human life. Individual choice was scorned and the patient subordinated to the whims of a criminal government. When considering the Nazi analogy and its relevance to medical ethics in our time, this critical difference should always be at the forefront of our analysis.
References
Aly, Götz, Peter Chroust, and Christian Pross, ed. (1994). Cleansing the Fatherland: Nazi Medicine and Racial Hygiene. Baltimore: The Johns Hopkins University Press, 1994.
Binding, Karl, and Alfred Hoche. (1920). Die Freigabe der Vernichtung lebensunwerten Lebens: ihr Mass und Ihre Form. Leipzig: Verlag von Felix Meiner.
Bock, Gisela. (1986). Zwangssterilization im Nationalsozialismus. Opladen.
Burleigh, Michael. (1994). Death and Deliverance: “Euthanasia” in Germany 1900-1945. Cambridge: Cambridge University Press.
Burleigh, Michael. (1991). The Racial State: Germany 1933-1945. Cambridge: Cambridge University Press.
Fest, Joachim C. (1974). Hitler. Trans. Richard and Clara Winston. New York: Harcourt Brace Jovanovich., Inc.
Friedlander, Henry. (1994). The Origins of Nazi Genocide: From Euthanasia to the Final Solution. Chapel Hill: The University of North Carolina Press.
Grodin, Michael A., Erin L. Miller, and Johnathan I. Kelly (2018). The Nazi Physicians as Leaders in Eugenics and “Euthanasia:” Lessons for Today. The American Journal of Public Health 108(1), 53-57.
Gould, Stephen Jay. (1996). The Mismeasure of Man. New York: W. W. Norton & Co.
Kevles, Daniel J. (1995). In the Name of Eugenics: Genetics and the Uses of Human Heredity. Cambridge: Harvard University Press.
Klee, Ernst. (2001). Dokumente zur “Euthanasie.” Frankfurt a.M.: Fischer.
Klee, Ernst. (1986). “Euthanasie” im NS-Staat: Die Vernichtung “lebensunwerten Lebens.” Frankfurt a.M.: Fischer.
Lammers, Hans Heinrich, Testimony of, 25 October 1945, NARA, M1270, Roll 11.
Lifton, Robert Jay. (1986). The Nazi Doctors: Medical Killing and the Psychology of Genocide. New York: The Free Press.
Lombroso, Cesare. (1887). L’homme criminal. Paris: F. Alcan.
Proctor, Robert N. (1988). Racial Hygiene: Medicine under the Nazis. Cambridge: Harvard University Press.
Spencer, Herbert. (1864). Social Statics. New York: D. Appleton & Co.
Taylor, Telford. (1946). Opening Statement at the Doctors Trial. Accessed August 8, 2022.
U. S. Holocaust Memorial Museum. No date. Holocaust Encyclopedia. United States Holocaust Memorial Museum “Euthanasia Program and Aktion T4”. Accessed August 8, 2022.
U. S. Holocaust Memorial Museum. No date. Holocaust Encyclopedia. United States Holocaust Memorial Museum “The Nuremberg Code”. Accessed August 8, 2022.
Weinberg, Gerhard., ed. (1961). Hitlers Zweites Buch. Stuttgart.
Weindling, Paul. (1989). Health, Race and German Politics Between National Unification and Nazism 1870-1945. Cambridge: Cambridge University Press.
Head of the US prosecution team at Nuremberg after Robert H. Jackson's resignation in 1946. Taylor led the American prosecution of the trials of Nazi war criminals subsequent to the International Military Tribunal. In this capacity, he prosecuted the Doctors Trial, among others. Wikipedia
A theory of "racial hygiene,” embraced and promoted by the Nazi German government, growing from a (now pseudo-) scientific movement that began at the turn of the 20th century. Eugenics “supporters lobbied for 'positive' eugenic efforts, including public policies... to maintain physically, racially, and hereditarily 'healthy' individuals... (including) motherhood training, and social welfare to 'deserving' families… Eugenics supporters hoped to encourage 'better' families to reproduce.” United States Holocaust Memorial Museum
A pseudoscientific "campaign to 'cleanse' German society of individuals viewed as biological threats to the nation’s 'health'. ” United States Holocaust Memorial Museum 2022
Disguised by the Latin term for “good death,” the Nazi program would select and kill people with disabilities, improving the ‘race’ and reducing financial and other burdens to society. ‘A rehearsal for... genocide.’ Rowman and Littlefield
Treaty signed between the Vatican and Nazi government on July 20, 1933. Wikipedia
Hitler's personal chancellery was "handling different issues pertaining to matters such as complaints against party officials, appeals from party courts, official judgments, clemency petitions by NSDAP fellows, and Hitler's personal affairs. The Chancellery of the Führer was also a key player in the Nazi euthanasia program." Wikipedia, 2022.
Organization created by Himmler in September 1939, combining the Security Police, Gestapo, Criminal Police, and Security Service. It was responsible for organizing some of the most destructive phases of the Holocaust, including the composition and deployment of the Einsatzgruppen and the creation/administration of the death camps. United States Holocaust Memorial Museum
The Nuremberg Code "is a set of ethical research principles for human experimentation created by the court in U.S. v Brandt, one of the Subsequent Nuremberg trials that were held after the Second World War." Wikipedia
